Diet 15 min read
Nutrition for Muscle Growth & Recovery: The Real Science
India ranks among the highest countries in the world for body fat percentage. It also ranks among the lowest for skeletal muscle mass. The 2024 InBody Global Report…
Reading about body composition? Find an InBody test centre near you →
India ranks among the highest countries in the world for body fat percentage. It also ranks among the lowest for skeletal muscle mass. The 2024 InBody Global Report analysed data from 17 countries over five years. It found that India, Chile, and Mexico have the highest body fat percentages globally. In contrast, countries with higher Skeletal Muscle Index (SMI) values maintain lower body fat across all age groups. For Indian adults, this creates a serious problem. The population already faces the thin-fat phenotype, protein-deficient diets, and the world’s highest burden of type 2 diabetes (T2DM). In this context, building muscle is not just a fitness goal. It is a metabolic necessity. It is a metabolic health imperative.
The science of skeletal muscle hypertrophy has advanced dramatically. Recent research (2023–2025) has clarified the key drivers of hypertrophy. These include training volume, protein intake, and progressive overload. It also highlights metabolic factors specific to Indian adults. These include high visceral fat, insulin resistance, and low baseline muscle mass. This article outlines seven science-backed strategies for building muscle. It also explains how InBody body composition analysis confirms whether each strategy is working.
| Highest BF% India, Chile, and Mexico have the highest body fat percentages globally in the 2024 InBody Report at every age group, in both men and women | 1.6–2.2 g/kg Daily protein intake required for maximum muscle hypertrophy nearly double the average Indian dietary intake and significantly above ICMR-NIN RDA of 0.83 g/kg | 10–20 sets Weekly volume per muscle group associated with maximum hypertrophy in the 2025 Pelland et al. meta-regression the most comprehensive training volume analysis published to date | 8–12 weeks Minimum period for measurable skeletal muscle mass increase to appear on InBody after initiating an evidence-based resistance training programme |
The India Muscle Problem: Why This Matters Clinically
India has one of the lowest average protein intakes globally. In contrast, the United States averages over 110 g per day. Protein is the primary substrate for muscle protein synthesis. Without it, hypertrophy cannot occur efficiently. As a result, many Indian adults train consistently but fail to build muscle. The limiting factor is not effort. It is inadequate nutritional support. The 7 science-backed strategies in this article address both the training and nutritional sides of this equation.
Low skeletal muscle mass is not a cosmetic concern. Skeletal muscle handles approximately 80% of insulin-stimulated glucose disposal, making it the primary determinant of metabolic health. Low Skeletal Muscle Index (SMI) is independently associated with elevated T2DM risk, cardiovascular mortality, hospitalisation, falls, fractures, and all-cause mortality. The Indian Consensus on Sarcopenia (2025) identified a critical risk. Asian Indians with T2DM have six times higher odds of low appendicular muscle mass. This creates a dangerous cycle. Low muscle mass worsens insulin resistance. Worsening diabetes accelerates further muscle loss. Together, these conditions reinforce each other and increase long-term disease risk.
THE THIN-FAT PARADOX AND MUSCLE BUILDING IN INDIA
The Indian thin-fat phenotype creates a uniquely challenging environment for muscle building. High visceral fat drives systemic inflammation (TNF-α, IL-6) that suppresses muscle protein synthesis. Fat-driven insulin resistance blocks the post-workout anabolic insulin response. Low skeletal muscle mass reduces glucose disposal capacity. It also lowers anabolic hormone sensitivity. This creates a poor environment for hypertrophy. In many cases, the body is metabolically disadvantaged before training even begins. InBody helps track this clearly. It measures both skeletal muscle mass and visceral fat in a single scan. This allows clinicians to monitor both barriers and outcomes simultaneously. Learn more about why BMI misses what body composition reveals.
Way 1 — Progressive Overload: The Non-Negotiable Foundation of Muscle Growth
Progressive overload, systematically increasing the mechanical stimulus placed on muscle over time, is the primary driver of skeletal muscle hypertrophy. Muscle grows when it is repeatedly subjected to a mechanical load it is not fully adapted to. Muscle growth requires progressive overload. Without it, adaptation does not occur. The biological response involves mTOR activation, satellite cell recruitment, and increased protein synthesis. Over time, this increases muscle fibre size. If the training stimulus does not increase, this cascade stops. Muscle growth stalls regardless of protein intake or consistency.
Progressive overload can be achieved in several ways. These include increasing load, repetitions, or total sets. It can also involve reducing rest time, improving range of motion, or increasing time under tension. Any of these variables can drive hypertrophy. The key is consistent and measurable progression.Evidence supports this. The 2025 Pelland et al. meta-regression showed that both training volume and frequency independently drive muscle growth. Optimal volume lies between 10–20 sets per muscle group per week.
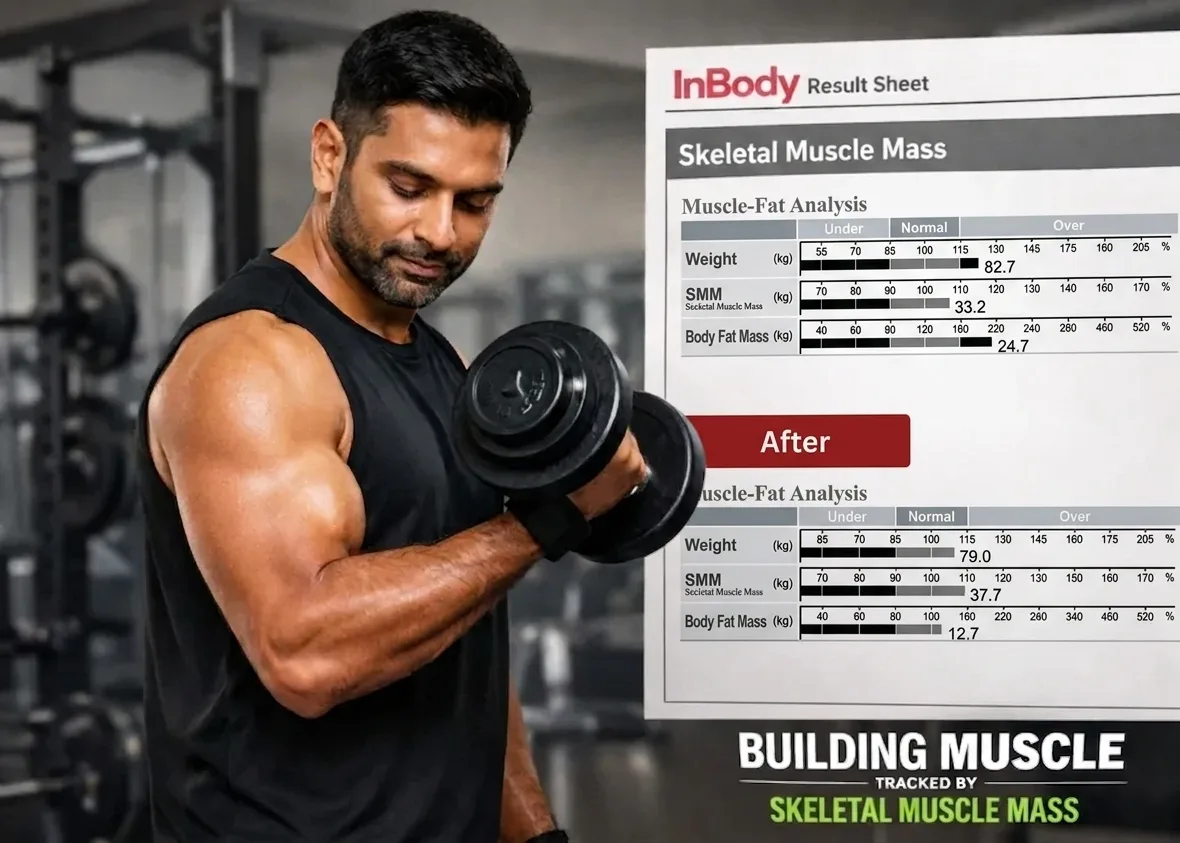
HOW INBODY CONFIRMS PROGRESSIVE OVERLOAD IS WORKING
Strength gains do not always equal muscle growth. Some gains are neuromuscular, not structural. This distinction matters. Gym performance alone cannot confirm hypertrophy. InBody solves this problem. It directly measures Skeletal Muscle Mass (SMM). This helps distinguish between neural adaptation and actual muscle growth. If SMM does not increase after 8–12 weeks, something is missing. The issue may be training volume, protein intake, or recovery.
Way 2 — Protein Intake: Getting the Dose Right for the Indian Context
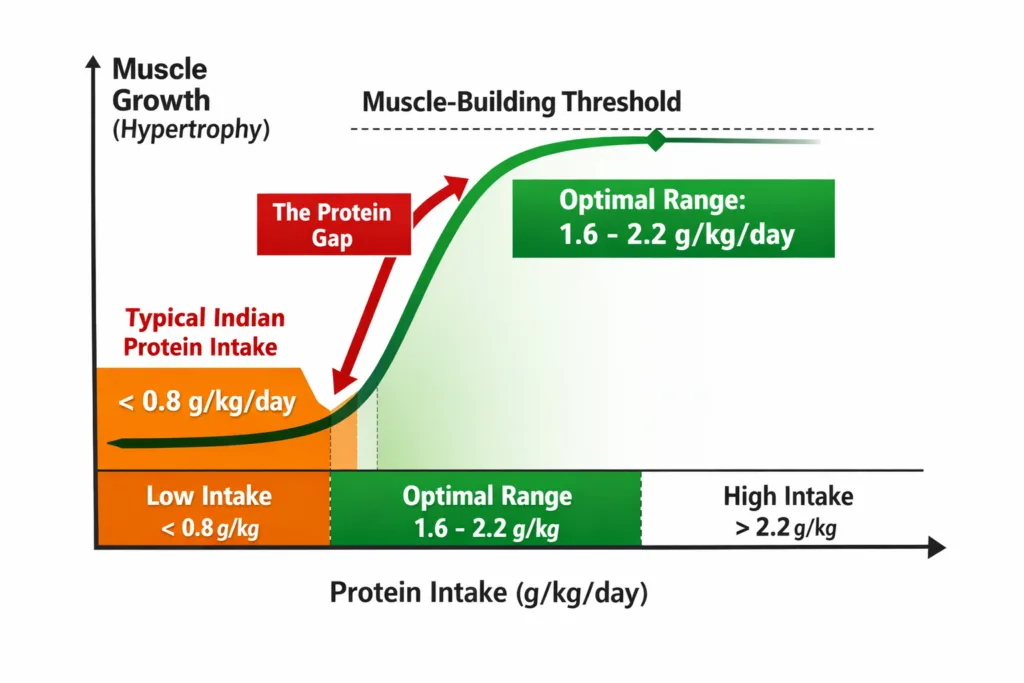
Protein is the substrate for muscle protein synthesis. Protein intake is essential for muscle growth. Without it, training cannot produce net muscle gain. A meta-analysis of 49 studies confirmed this. Protein supplementation significantly increases fat-free mass. Benefits plateau around 1.62 g/kg/day. More recent evidence suggests up to 2.2 g/kg/day may be optimal. This is especially true for individuals with higher body fat or insulin resistance.
For Indian adults, this creates a specific clinical challenge. The ICMR-NIN 2020 RDA for protein is 0.83 g/kg/day set for sedentary adults to prevent deficiency, not to optimise hypertrophy. Average Indian dietary protein intake falls significantly below even this conservative threshold in many population groups. The gap between current intake and optimal intake is large. It is also poorly recognised. Most Indian diets fall well below 1.6 g/kg/day. Even standard clinical advice often underestimates requirements. The Indian Consensus on Sarcopenia recommends 1.2–1.5 g/kg/day as a minimum. This is for preservation, not hypertrophy. For muscle growth, a higher intake is essential.
PROTEIN TIMING: THE ADDITIONAL EVIDENCE
Protein timing also matters. Muscle protein synthesis peaks for 3–4 hours after training. Consuming 20–40 g of high-quality protein within two hours post-workout improves outcomes. Total intake, distribution, and protein quality all influence results. InBody provides outcome validation. Changes in SMM confirm whether intake strategies are effective
Way 3 — Training Volume: The Dose-Response Relationship That Most Programmes Miss
Training volume has a strong dose-response relationship with hypertrophy. More volume produces more growth, up to a threshold. Evidence suggests 10–20 sets per muscle group per week is optimal. Many Indian trainees fall below this range. This leads to suboptimal results despite consistent effort.
Small increases in volume can produce measurable gains. Adding 3–5 sets per week can shift results significantly. Training frequency also matters. Muscles trained 2–3 times per week grow more than those trained once weekly. Distributing volume improves both recovery and adaptation.
TRAINING FREQUENCY: WHAT THE 2025 EVIDENCE CONFIRMS
The 2025 meta-regression also confirmed that training frequency independently contributes to hypertrophy, with muscles trained 2–3 times per week showing greater hypertrophy than once per week, when total volume is equated. This has direct programme design implications for Indian fitness settings: spreading volume across 2–3 sessions per week for each major muscle group is superior to concentrating all volume in a single weekly session, a finding that should change how most Indian gym programmes are designed for hypertrophy-focused clients.
Way 4 — Visceral Fat Reduction: Fixing the Biochemical Environment First
This is the strategy most fitness and clinical professionals overlook, and it is the one most specifically relevant to India. Building muscle in an environment of elevated visceral fat is biochemically inefficient. Visceral fat drives TNF-α and IL-6, which suppress mTOR signalling the primary anabolic pathway activated by resistance training. It drives insulin resistance that blunts the post-workout anabolic insulin response. It suppresses GH, testosterone, and IGF-1, the three hormones most important for muscle hypertrophy.
For Indian adults with a visceral fat level above 10 on InBody, targeting visceral fat reduction alongside resistance training produces significantly better muscle-building outcomes than resistance training alone. The practical implementation is a combination of HIIT for visceral fat reduction, dietary carbohydrate quality improvement (replacing refined carbohydrates with high-fibre whole food alternatives), and SGLT-2 inhibitors for patients with concurrent T2DM, all of which produce measurable VFL reduction that InBody tracks at every visit. As VFL falls from 12 toward 9 or below, the inflammatory suppression of muscle protein synthesis diminishes, and the same resistance training programme that was producing limited hypertrophy begins producing measurably greater gains.
CLINICAL IMPLICATION
For any Indian patient or client with a Visceral Fat Level above 10, the first 6–8 weeks of a muscle-building programme should include a visceral fat reduction component, not just resistance training. InBody’s simultaneous VFL and SMM tracking confirms whether this dual-target approach is working: VFL declining while SMM begins to increase is the ideal trajectory. VFL staying elevated while SMM barely changes is the signal that the inflammatory environment requires more aggressive attention before hypertrophy can proceed efficiently.
Way 5 — Sleep and Recovery: The Anabolic Window Most Indians Are Missing
The majority of muscle protein synthesis from a resistance training session occurs not during the session but in the 24–48 hours afterwards, during rest and sleep. Growth hormone is secreted in pulses predominantly during slow-wave sleep. Muscle repair, satellite cell proliferation, and myofibrillar protein synthesis all occur at the highest rates during sleep. Cortisol, the primary catabolic hormone that breaks down muscle protein, is suppressed during adequate sleep and elevated during sleep deprivation.
Sleep deprivation is associated with elevated TNF-α and IL-6, impaired GH secretion, elevated cortisol, and reduced insulin sensitivity, all of which independently suppress muscle protein synthesis and promote muscle catabolism. For Indian adults managing demanding work schedules, extended commutes, and high chronic stress burden, sleep duration and quality are frequently below the 7–9 hours per night that optimise the post-workout anabolic environment. The practical clinical implication is direct: a patient who is training and eating correctly but sleeping 5–6 hours per night is operating with a chronically activated catabolic hormonal profile, which InBody’s rising ECW/TBW ratio, a marker of systemic inflammatory stress, may begin to reflect before the scale or gym performance does.
KEY INSIGHT
InBody’s ECW/TBW ratio is a sensitive marker of systemic inflammatory and metabolic stress. In a client who is training consistently, eating adequately, and not building muscle, a rising or elevated ECW/TBW ratio is a clinical signal of unresolved inflammatory stress, potentially from inadequate sleep, chronic psychological stress, or undiagnosed metabolic disease. This is clinical data that no gym performance metric, dietary assessment, or body weight measurement can provide.
Way 6 — Segmental Training: Targeting the Muscle Deficits That Limit Overall Growth
Most resistance training programmes are designed for generic muscle development. They do not account for the specific muscle mass deficits of the individual patient or client. For Indian adults, where the 2024 InBody Global Report confirms that India has among the lowest Skeletal Muscle Index values for both men and women globally, the most efficient path to muscle growth is targeted intervention at the specific body segments most deficient in muscle mass.
InBody’s Segmental Lean Analysis provides the clinical data to make this possible. It measures skeletal muscle mass in each limb separately, right arm, left arm, right leg, left leg, and trunk and compares each to the population norm for the patient’s height and weight. A patient who shows within-range arm muscle mass but significantly below-norm leg muscle mass,, common in sedentary Indian professionals who walk limited distances and sit for extended periods has a specific training prescription: lower-body dominant resistance training prioritising quadriceps, hamstrings, and hip extension patterns. This targeted approach produces faster, measurable SMM gains than a generic programme because it applies the highest training stimulus to the segments with the greatest growth potential.
LEG MUSCLE MASS AND METABOLIC HEALTH IN INDIA
Leg muscles, the quadriceps, hamstrings, and gluteal muscles account for approximately 60–70% of total skeletal muscle mass and handle the majority of insulin-stimulated glucose disposal. Below-norm leg muscle mass is both a metabolic disease risk factor and a primary target for muscle-building interventions in Indian adults. InBody’s segmental lean analysis for the lower limbs is the clinical foundation for designing lower-body dominant programmes that produce the greatest metabolic and hypertrophic benefit simultaneously.
Way 7 — Serial Tracking: Measuring What You Are Building, Not Just What You Are Doing
The seventh and most practically important science-backed way to build muscle is to measure whether your programme is actually building it. This sounds self-evident, and yet the overwhelming majority of Indian gym-goers, fitness programme participants, and even clinical patients on muscle-building protocols have no objective data confirming whether skeletal muscle mass is increasing, decreasing, or unchanged. They track their scale weight, count their sets and log their protein. But none of these metrics directly measures what they are trying to achieve.
InBody serial assessment every 8–12 weeks for most individuals provides the data that closes this measurement gap. When a client’s InBody shows that SMM has increased by 1.4 kg over 12 weeks, their programme is working. SMM is unchanged after 12 weeks of consistent training and adequate protein; the programme requires modification to include more volume, better sleep, lower visceral fat, or increased dietary protein. When SMM is decreasing despite training, something is actively working against muscle growth: elevated inflammation, medication side effects, protein deficiency, or a metabolic disease that requires clinical evaluation.
INBODY SERIAL TRACKING: THE EVIDENCE FOR OUTCOMES
The most important strategy is measurement. Without it, progress cannot be confirmed. Most individuals rely on weight or mirror changes. These are unreliable indicators of muscle growth. InBody provides objective data. It shows whether SMM is increasing, stable, or declining. The mechanism: objective, specific, personal feedback creates intrinsic motivation and precise programme adjustment. If SMM does not increase after 12 weeks, the programme needs adjustment. Possible issues include low protein intake, insufficient volume, poor sleep, or high inflammation. If SMM decreases, a deeper clinical issue may be present. It sustains the adherence that produces the long-term hypertrophy that changes metabolic health.
What InBody Measures to Track Muscle Building: The Complete Picture
Each InBody scan delivers the following body composition metrics relevant to muscle building in under 60 seconds, at every visit:
| InBody Metric | What It Measures | Why It Matters for Muscle Building |
|---|---|---|
| Skeletal Muscle Mass (SMM) | Total lean muscle in kg per body segment | The primary outcome metric. Direct confirmation that resistance training and protein intake are producing measurable hypertrophy distinguishable from fluid or fat changes |
| Skeletal Muscle Index (SMI) | Appendicular skeletal muscle mass normalised for height | Assesses muscle mass against population norm. Identifies sarcopenia and sets the clinical baseline for muscle-building programme targets |
| Segmental Lean Analysis | SMM per limb right/left arm, right/left leg, trunk | Identifies specific muscle deficits per limb enabling targeted exercise prescription for the segments most deficient and most responsive to training |
| Body Fat Percentage | Fat mass as % of total body weight | Confirms that weight gain is from muscle (BF% falling or stable), not fat (BF% rising), the critical distinction scale weight cannot make |
| Visceral Fat Level (VFL) | Fat surrounding internal organs 1 to 20 scale | Confirms the anabolic environment is improving. VFL declining confirms inflammatory suppression of muscle protein synthesis is being reduced |
| Phase Angle | BIA-derived marker of cellular membrane integrity | Rises with muscle growth and improved cellular health. A rising phase angle alongside rising SMM is the dual confirmation of genuine hypertrophy, not fluid gain |
Real Case: The IT Professional Who Finally Built Muscle After 3 Years of Trying
A 34-year-old male software architect in Bengaluru had been training at a gym for 3 years. A 78 kg male trained four times per week. He consumed about 80–90 g of protein daily.
After three years, his weight increased by 2.8 kg. However, his physique and strength plateaued. InBody revealed the issue. His protein intake was only 1.03 g/kg/day, visceral fat was elevated, and his leg muscle mass was below normal. His programme was redesigned. Protein was increased to 1.7 g/kg/day. Lower-body training volume was doubled. HIIT was added.
Within weeks, measurable muscle gain was observed. At his 12-week InBody scan:
| +2.3 kg Skeletal Muscle Mass gaine more than in the preceding 3 years combined | ↓2 units Visceral Fat Level (10 → 8) | ↑0.5° Phase Angle improvement (5.0° → 5.5°) | ↓3.1% Body Fat Percentage reduced |
His scale weight changed by 0.9 kg. His strength hit new all-time records in squat, Romanian deadlift, and leg press within 10 weeks. For the first time in 3 years, he had objective data confirming he was building muscle and the data showed him exactly what had been blocking it for 36 months.
Frequently Asked Questions
Q. How much protein do Indians need to build muscle?
The ICMR-NIN 2020 RDA of 0.83 g/kg/day is set for sedentary adults to prevent deficiency, not to optimise hypertrophy. For muscle building, the evidence supports 1.6–2.2 g/kg/day of total protein. For sarcopenia treatment, the Indian Consensus on Sarcopenia (2025) recommends a minimum of 1.2–1.5 g/kg/day. The 2024 InBody Global Report found that India has among the lowest daily protein intake globally, creating a significant gap between typical Indian dietary protein and the muscle-building threshold. InBody’s SMM tracking confirms whether a patient’s specific protein intake is translating into measurable hypertrophy.
Q. Why is building muscle harder for Indian adults?
Three factors make muscle building specifically harder for Indian adults. First, the thin-fat phenotype: higher body fat at the same BMI as Western populations, with visceral fat driving insulin resistance that suppresses muscle protein synthesis. Second, protein intake: average Indian diets are significantly below the 1.6–2.2 g/kg/day required for hypertrophy. The 2024 InBody Global Report confirms India has among the lowest protein intake globally. Third, metabolic disease prevalence: India’s 101 million T2DM patients face 6-fold higher odds of low appendicular skeletal muscle mass, and the inflammation from concurrent visceral obesity systematically limits hypertrophy without targeted intervention.
Q. How does InBody help track muscle building progress?
InBody tracks muscle building through six key metrics: Skeletal Muscle Mass (SMM) the primary outcome; Segmental Lean Analysis SMM per limb to identify specific deficits; InBody Score overall body composition quality trajectory; Visceral Fat Level confirms the inflammatory environment is improving; Body Fat Percentage confirms weight gain is from muscle not fat; and Phase Angle rises as muscle grows and cellular function improves. Together, these six metrics provide the complete muscle-building progress picture that scale weight and gym performance alone cannot deliver.
Key Takeaways
- India has high body fat and low muscle mass. This makes muscle building a metabolic priority.
- Effective strategies include progressive overload, adequate protein, optimal volume, fat reduction, sleep, targeting, and tracking.
- Protein intake remains the biggest gap in India.
- Visceral fat must be reduced for efficient hypertrophy.
- Segmental analysis enables precise training.
- InBody provides fast, objective, and actionable data.
Track Every Kilogram of Muscle You Build
An InBody scan provides a complete picture. It measures muscle, fat, and cellular health in under 60 seconds. More importantly, it shows whether your programme is working. If it is not, it shows exactly what to change.

Find an InBody Scanner Near You
References & Further Reading
- InBody Global Report 2024. Body fat percentage and SMI by country — India among highest BF%, lowest SMI. InBody. 2024.
- Nutritional interventions for muscle hypertrophy — scientometric analysis 1992–2025. PMC12317481. 2025.
- Pelland J et al. Resistance Training Dose-Response: Meta-Regressions on Volume and Frequency for Hypertrophy and Strength. SportRχiv. 2025.
- Morton RW et al. A systematic review, meta-analysis and regression of the effect of protein supplementation on resistance training-induced gains in muscle mass. Br J Sports Med. 2018;52(6):376–384.
- Kalra S et al. Indian Consensus on Sarcopenia — T2DM, Asian Indian low muscle mass odds, protein recommendations. Int J Gen Med. 2025;18:1731–1745.
- Colleluori G et al. Sarcopenic obesity — insulin resistance, adipokine/myokine crosstalk, intramuscular fat. Frontiers in Endocrinology. 2020.

Most trending articles

Diet Mistakes That Stall Muscle Growth (And How to Fix Them)
Those with modest appetites, slim bodies, or high metabolisms may find it difficult to gain weight. The secret to gaining weight is to consume more calories than your…

Weight Loss vs Fat Loss: What’s the Real Difference?
When people say they want to lose weight, what they often mean is losing fat. However, weight loss and fat loss are not the same, and understanding the…
Are Artificial Sweeteners Safe for Diabetics? An Honest Look
If you have diabetes, you’ve likely experienced that frustrating moment when you really want adrink, but you’re browsing an aisle full of “sugar-free” options, and you’re not sure what…