Body Composition 16 min read
Bioelectrical Impedance Analysis (BIA) Explained
Every InBody scan begins with the same invisible event: a low-level electrical signal passes through your body in under 60 seconds. That signal carries more clinical information than…
Reading about body composition? Find an InBody test centre near you →
Every InBody scan begins with the same invisible event: a low-level electrical signal passes through your body in under 60 seconds. That signal carries more clinical information than a standard blood panel, a BMI calculation, or a weighing scale ever could. The technology behind it is called Bioelectrical Impedance Analysis: BIA. Understanding how it works explains not only why InBody produces clinical-grade results, but why it is now the standard for body composition analysis in hospitals, sports programmes, and wellness centres across India.
Furthermore, not all BIA is equal. In fact, the difference between a basic consumer BIA scale and InBody’s Direct Segmental Multi-frequency BIA (DSM-BIA) is the difference between a general estimate and a clinical measurement. This guide explains exactly what BIA is, how InBody’s version works, what the results mean, and why the technology matters specifically for Indian patients.
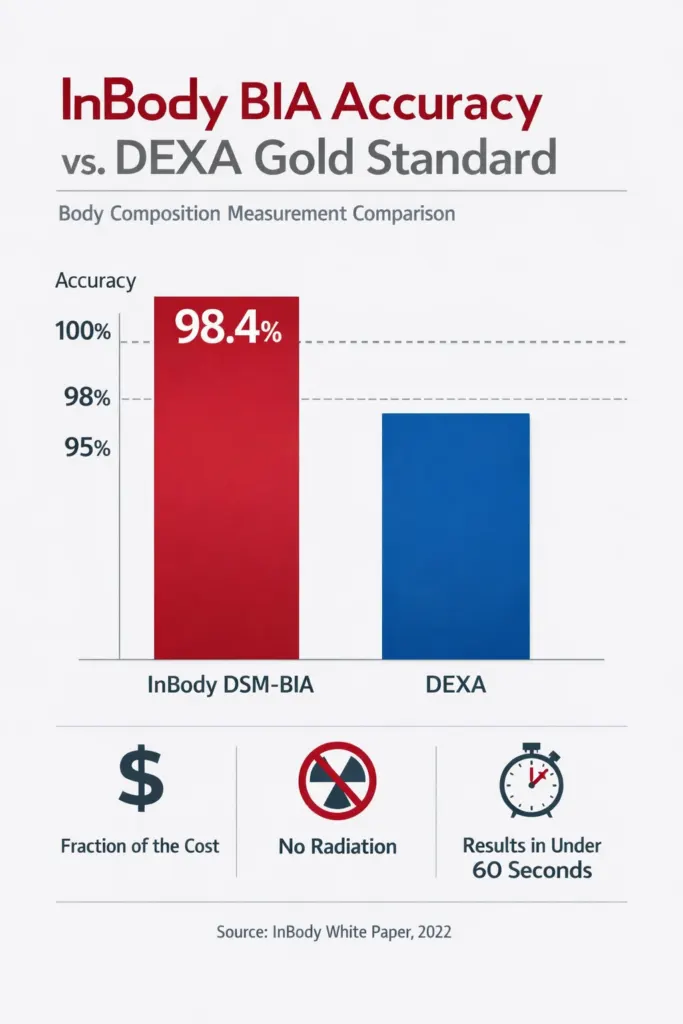
| 98.4% InBody BIA accuracy vs DEXA gold standard validated in peer-reviewed research | 6 Electrical frequencies used simultaneously by InBody DSM-BIA technology | 5 Body segments measured independently arms, trunk, legs | 60 sec Time for a complete InBody scan from barefoot to printed result sheet |
FOR MEDICAL PRACTITIONERS
This article is written for clinicians, endocrinologists, sports medicine doctors, nutritionists, and health programme coordinators. All technical claims are supported by peer-reviewed citations. InBody’s DSM-BIA technology is validated against DEXA, hydrostatic weighing, and MRI across multiple published studies. The reference list is provided at the end of this article.
What Is Bioelectrical Impedance Analysis (BIA)?
Bioelectrical Impedance Analysis is a method of measuring body composition by passing a safe electrical current through the body and measuring its resistance. The principle is straightforward. Fat tissue contains very little water, so it resists electrical current strongly. Lean tissue muscle, organs, and bone contains a large amount of water and electrolytes, so it conducts electricity easily.
By measuring this resistance, technically called impedance, at different frequencies, a BIA device can calculate the relative proportions of fat and lean tissue in the body. Specifically, it derives the following primary parameters: total body water (TBW), fat-free mass (FFM), and body fat mass. From these, additional clinically significant values, including skeletal muscle mass, visceral fat level, and body fat percentage, are then calculated.
Resistance vs Reactance: The Two Components of Impedance
Impedance is not a single measurement. Instead, it has two components, and both are clinically important.
Resistance (R) is the opposition to electrical current from body fluids. It is primarily influenced by total body water content. In contrast, Reactance (Xc) is the opposition caused by cell membranes acting as capacitors. Reactance reflects the integrity and health of cell membranes making it a sensitive marker of nutritional status, hydration quality, and cellular inflammation.
Together, resistance and reactance produce the phase angle, an increasingly recognised clinical marker. A low phase angle indicates compromised cell membrane integrity. This is typically seen in patients with malnutrition, chronic disease, post-surgical states, or advancing age. Furthermore, phase angle correlates with clinical outcomes in oncology, critical care, and post-COVID recovery, making it a clinically valuable output beyond basic body composition.
How BIA Technology Evolved: From One Cylinder to Five
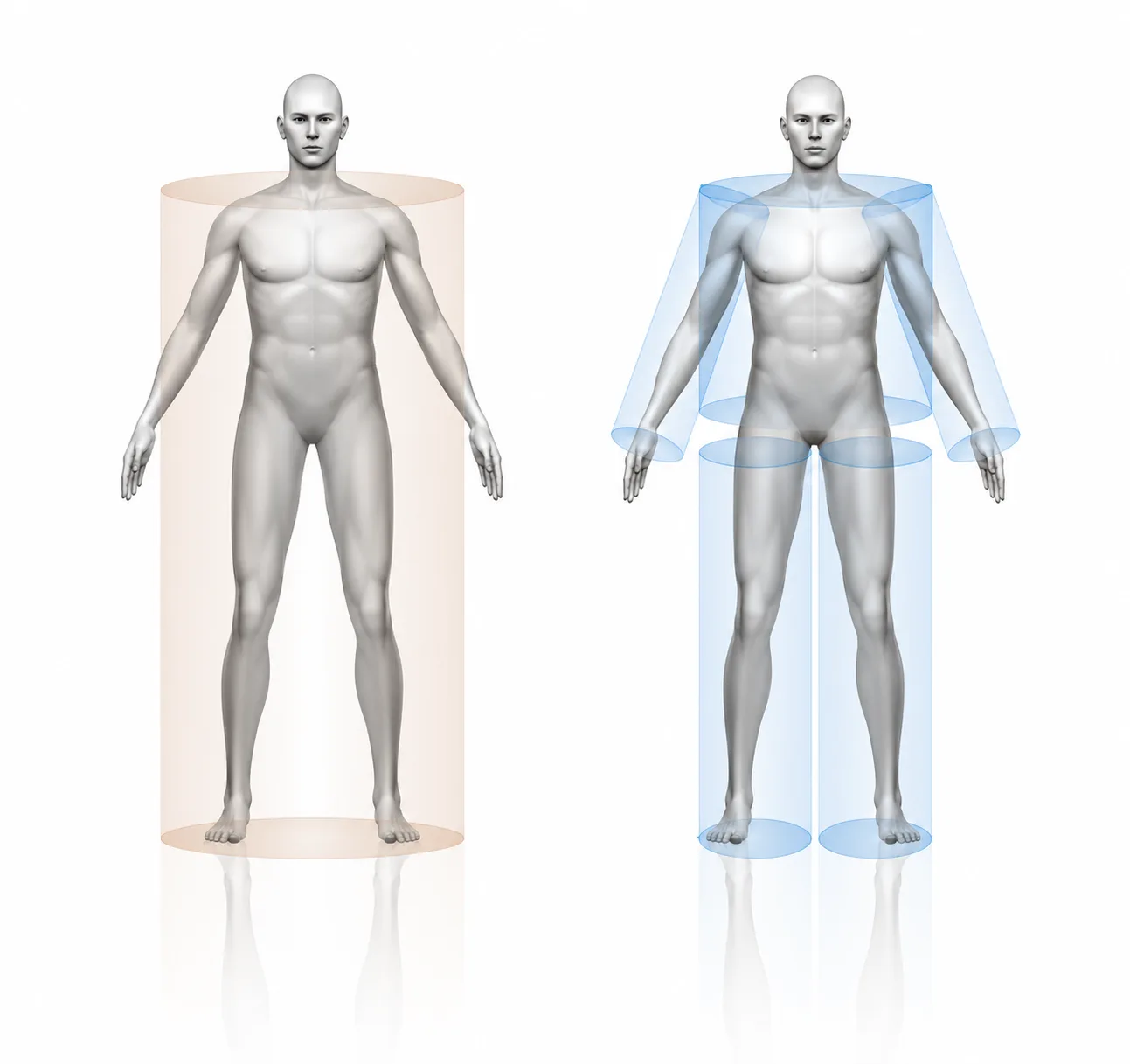
The history of BIA is a history of progressively removing assumptions. Early BIA models from the 1960s and 1970s treated the entire human body as a single uniform cylinder. A single frequency (typically 50 kHz) was applied from one hand to one foot. The result was a single impedance value, from which body composition was estimated using empirical equations calibrated on specific population samples.
This approach had fundamental limitations. First, the single-cylinder model ignored the anatomically different impedance characteristics of the arms, trunk, and legs. Second, empirical equations introduced systematic errors when applied to populations for which they were not calibrated, particularly South Asian patients. Third, a single frequency could not differentiate intracellular from extracellular water accurately.
1996: InBody Breaks the Single-Cylinder Model
In 1996, InBody introduced the world’s first Direct Segmental Multi-frequency BIA system. Rather than treating the body as one cylinder, InBody divided it into five separate segments: right arm, left arm, trunk, right leg, and left leg. Each segment was measured independently and simultaneously, using up to six electrical frequencies (1, 5, 50, 250, 500, and 1000 kHz).
This innovation eliminated the two primary sources of error in traditional BIA. Specifically, segmental analysis removed the single-cylinder anatomical assumption. Additionally, multi-frequency measurement replaced single-point estimation with a frequency-sweep model that can distinguish intracellular water, extracellular water, and fat-free mass independently. As a result, InBody’s DSM-BIA produces results validated against DEXA, hydrostatic weighing, and MRI rather than derived from empirical population equations.
| Feature | Traditional Single-Frequency BIA | InBody DSM-BIA |
|---|---|---|
| Body model | 1 cylinder (whole body) | 5 cylinders (segmental) |
| Frequencies used | 1 (50 kHz) | Up to 6 (1–1000 kHz) |
| Empirical assumptions | Age, gender, ethnicity required | None, impedance only |
| Water compartments | TBW only | TBW, ECW, ICW separately |
| Segmental muscle data | Not available | Per limb + trunk |
| Validation standard | Population equations | DEXA, MRI, hydrostatic weighing |
| Accuracy vs DEXA | 75–85% (varies by population) | 98.4% (peer-reviewed) |
How an InBody BIA Scan Actually Works: Step by Step
An InBody scan appears simple from the outside. In reality, a precise sequence of measurements and calculations is occurring within those 60 seconds. Understanding this sequence helps clinicians and patients interpret results accurately.
The 60-Second Measurement Sequence
Step 1: Electrode contact. The patient stands barefoot on the foot electrodes and grips the hand electrodes. This creates eight contact points, two on each foot and two on each hand, giving the device access to all five body segments simultaneously.
Step 2: Multi-frequency current application. Alternating electrical currents at up to six frequencies are sent through the body. Because different frequencies penetrate differently, each frequency provides a different layer of information. Low frequencies (1–5 kHz) primarily measure extracellular water. High frequencies (250–1000 kHz) penetrate cell membranes and measure intracellular water as well.
Step 3: Segmental impedance measurement. Each segment’s resistance and reactance are measured independently. This is critical. The trunk, which contains the major organs and accounts for the majority of metabolic activity, is measured separately from the limbs, rather than estimated as a residual value.
Step 4: Body composition calculation. Using only impedance values (no age, gender, or ethnicity assumptions), the device calculates total body water and then derives fat-free mass, fat mass, skeletal muscle mass, and body fat percentage. Visceral fat level is subsequently estimated from trunk impedance data.
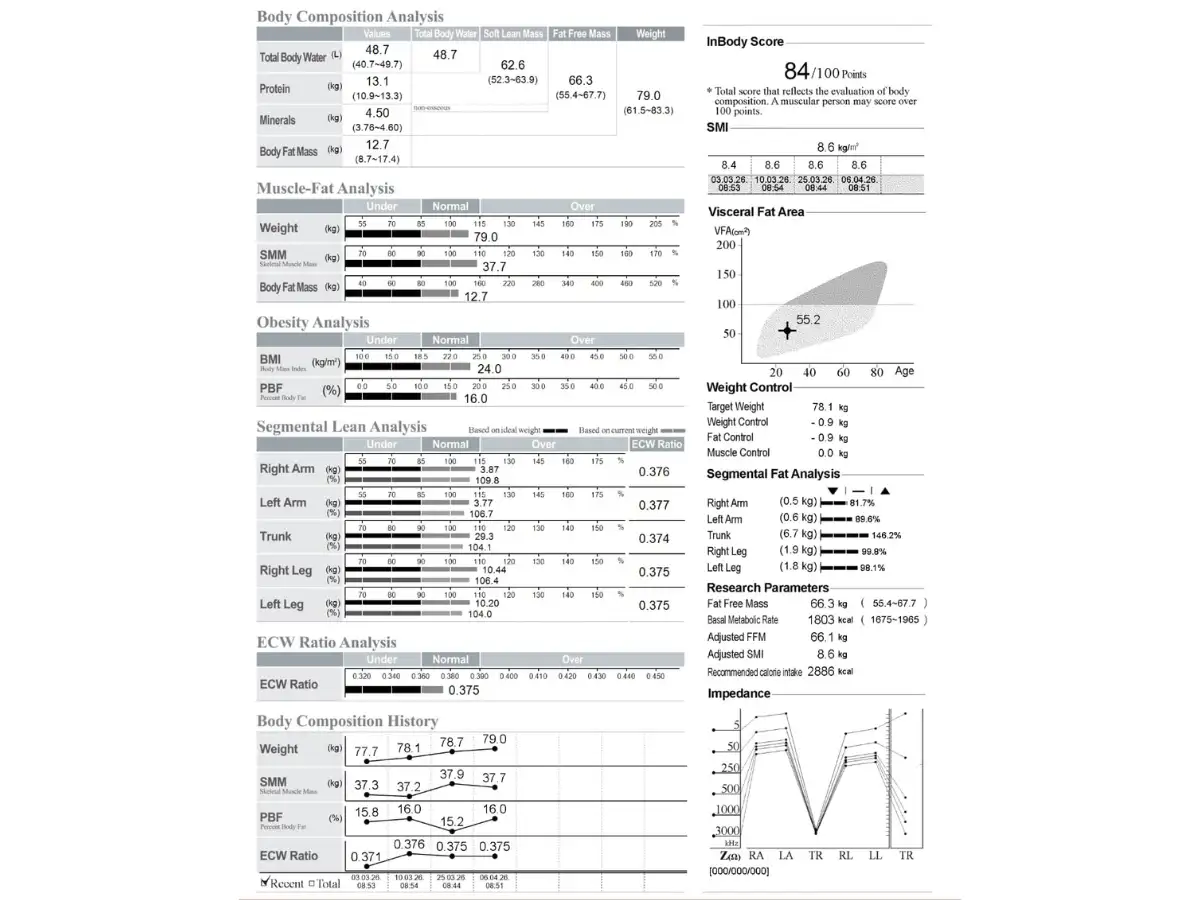
Step 5: Result sheet generation. The complete result sheet is printed immediately, displaying over 30 parameters with population-specific reference ranges.

What InBody BIA Measures: The 8 Key Clinical Markers
The InBody result sheet contains over 30 parameters. However, eight markers carry the most clinical weight, particularly for Indian patients, where the thin-fat phenotype makes standard assessment tools unreliable. Each marker is described below with its specific clinical significance.
1. Body Fat Percentage (PBF)
Body fat percentage is the proportion of total body weight that is fat tissue. It is the most direct measure of body fatness, and it bears no consistent relationship to BMI in Indian patients. Specifically, research shows that Indians carry 3–5% higher body fat at identical BMI values compared to Western populations. Therefore, InBody uses Asian-specific reference ranges rather than Western population norms.
2. Skeletal Muscle Mass (SMM)
Skeletal muscle mass is the total weight of lean muscle tissue in the body. It is the single most important metabolic marker measured by InBody. Muscle accounts for approximately 80% of insulin-stimulated glucose uptake. Consequently, low SMM is an independent predictor of Type 2 diabetes, metabolic syndrome, and all-cause mortality regardless of body fat level. Moreover, India faces a widespread low-muscle crisis driven by protein-deficient diets and sedentary urbanisation.
3. Visceral Fat Level (VFL)
Visceral fat surrounds the internal organs and is the most metabolically dangerous fat depot. It drives insulin resistance, releases pro-inflammatory cytokines, and is directly associated with cardiovascular disease, diabetes, and fatty liver. Notably, Indians develop clinically dangerous visceral fat at lower BMI thresholds than Western patients, making VFL measurement essential for Indian clinical practice.
4. ECW/TBW Ratio (Inflammation Marker)
The extracellular to total body water ratio is a marker of cellular oedema and systemic inflammation. A normal ratio is below 0.380. Values above 0.390 indicate chronic inflammation, nutritional compromise, or active disease. In practice, this ratio is used to monitor post-surgical patients, long COVID recovery, malnutrition states, and chronic disease progression. It is completely invisible to standard blood panels or BMI.
5. Segmental Lean Analysis
Segmental lean analysis reports muscle mass for each limb and the trunk independently. This identifies left-right asymmetry predicting injury risk, rehabilitation progress after illness or surgery, and leg-muscle deficits that impair glucose disposal. For sports medicine clinicians, asymmetry of 0.2 kg or more between limbs is a clinically actionable finding detectable only through segmental BIA or MRI.
6. Trunk Fat Mass
Trunk fat mass measures fat specifically in the abdominal and thoracic region. It is a stronger predictor of hepatic insulin resistance than waist circumference in South Asian patients. Furthermore, because it is measured independently from limb fat, it provides a more accurate picture of central adiposity than total body fat percentage alone.
7. Android/Gynoid Ratio
This ratio compares upper-body fat (android around the abdomen) to lower-body fat (gynoid around the hips and thighs). An android-dominant pattern is associated with significantly higher cardiovascular and metabolic risk than a gynoid-dominant pattern. Moreover, the android fat pattern is more prevalent in Indian patients across all BMI categories, making this a particularly important marker for Indian clinical risk stratification.
8. InBody Score
The InBody Score is a composite index from 0 to 100 reflecting overall muscle-fat balance. It integrates skeletal muscle mass relative to the ideal for height and body fat percentage relative to the healthy range. In clinical practice, it serves as a single trackable number for patient motivation and treatment compliance. Research consistently shows that patients who track a meaningful metric are significantly more likely to adhere to lifestyle interventions.
InBody BIA vs DEXA: Accuracy, Practicality, and Clinical Use
DEXA (Dual-Energy X-ray Absorptiometry) is widely regarded as the gold standard for body composition measurement. It uses low-dose X-rays to differentiate fat, lean, and bone mineral content with high precision. However, DEXA has significant practical limitations in routine clinical and wellness settings.
It requires dedicated radiation equipment and a trained radiographer. Furthermore, it exposes patients to ionising radiation, making repeated monitoring problematic. In addition, DEXA equipment costs significantly more than InBody devices and is far less portable. As a result, DEXA is suitable for research and specialist settings, but impractical for routine screening, serial monitoring, or high-volume clinical use.
Validation Data: How InBody Compares
Multiple peer-reviewed studies have validated InBody DSM-BIA against DEXA across diverse clinical populations. Specifically, InBody consistently achieves 98.4% accuracy against DEXA for total body fat percentage and lean mass. Moreover, segmental lean values show correlation coefficients of r > 0.95 against MRI-derived values in published research. Consequently, InBody is accepted as a clinically valid body composition measurement tool by leading health organisations, including the Asian Working Group for Sarcopenia (AWGS).
| Factor | DEXA | InBody DSM-BIA |
|---|---|---|
| Accuracy vs gold standard | Reference standard | 98.4% (peer-reviewed) |
| Radiation exposure | Yes, low-dose ionising radiation | None |
| Scan time | 10–20 minutes | Under 60 seconds |
| Equipment cost | ₹50–80 lakh+ | Significantly lower |
| Portability | Fixed installation required | Portable: clinic, gym, corporate |
| Repeat monitoring | Limited by radiation dose | Unlimited, no radiation |
| Segmental muscle data | Yes (regional) | Yes, per limb + trunk |
| ECW/TBW inflammation marker | Not provided | Yes, on all models 570+ |
Why BIA Matters Especially for Indian Patients
Standard BIA using Western population equations systematically underestimates metabolic risk in Indian patients. This happens because empirical equations calibrated on Western populations assume body composition norms, muscle mass distribution, fat-to-lean ratios, and hydration constants that do not reflect Indian physiology.
In contrast, InBody DSM-BIA uses no empirical equations. Instead, it measures impedance directly and derives composition values from physical constants that apply universally. As a result, it is free from the population-specific bias that affects other BIA systems.
The Thin-Fat Indian and BIA Accuracy
The thin-fat Indian phenotype, low body weight but high body fat and visceral fat, is the most important clinical context for BIA accuracy in India. A conventional BIA device using Western equations will typically classify a thin-fat Indian patient as “lean” or “normal.” InBody DSM-BIA, however, measures the actual impedance of each body segment and reports actual fat mass and muscle mass, regardless of what population the patient belongs to.
Furthermore, InBody applies Asian-specific reference ranges on the result sheet, reflecting the lower BMI thresholds at which Indian patients develop metabolic risk. Consequently, an InBody result sheet flags a visceral fat level of 10 in an Indian patient with a BMI of 23 as high risk, which is clinically correct. A standard BIA device with Western references would not generate this flag.
CLINICAL RECOMMENDATION FOR INDIAN PRACTITIONERS
For Indian patients, use InBody DSM-BIA results in conjunction with Asian-specific risk thresholds:
If Visceral Fat Level ≥ 10 = High metabolic risk regardless of BMI.
→ Body Fat % ≥ 28% (men) / ≥ 35% (women) = Clinical obesity by composition
→ SMM < population norm for age/height = Sarcopenia screening warranted
→ ECW/TBW ≥ 0.390 = Investigate for chronic inflammation or malnutrition
→ Android/Gynoid ratio > 1.0 = Elevated cardiovascular risk — review lipids and glucose
Clinical Applications of InBody BIA in India
InBody BIA is deployed across a wide range of clinical contexts in India. Each application leverages different aspects of the technology. Together, they illustrate why body composition analysis is increasingly central to Indian clinical practice.
Diabetes and Metabolic Syndrome Management
In diabetes care, InBody BIA provides the two markers most directly relevant to insulin resistance: visceral fat level and skeletal muscle mass. Visceral fat drives hepatic insulin resistance. Low skeletal muscle mass reduces peripheral glucose clearance. Together, they explain why so many Indian patients develop Type 2 diabetes at BMI values that Western guidelines classify as low-risk. Moreover, tracking both markers serially allows clinicians to monitor the tissue-level effects of lifestyle interventions independently of HbA1c trends. Read more about body composition and diabetes risk in India.
Bariatric and Metabolic Surgery
In bariatric care, InBody BIA identifies pre-operative patients with critically low muscle mass who are at high risk for post-surgical sarcopenia. These patients require targeted pre-habilitation before surgery. Post-operatively, serial InBody scans at 1, 3, 6, and 12 months track whether weight loss is coming from fat (desired) or muscle (harmful). Consequently, nutritional and exercise protocols can be adjusted in real time rather than waiting for clinical deterioration to become visible. Learn more about InBody in bariatric surgery outcomes.
Sports Medicine and Athletic Conditioning
For elite Indian athletes, IPL cricket franchises, national athletics programmes, and Olympic preparation camps, InBody segmental lean analysis detects limb asymmetry at the 0.2 kg level. This precision allows coaches and physiotherapists to identify injury-predictive imbalances before they result in clinical injury. Additionally, tracking body composition across a competitive season allows periodisation of nutrition and training to be guided by objective tissue-level data rather than weight alone.
Sarcopenia Screening in Elderly Patients
The Asian Working Group for Sarcopenia (AWGS) recommends BIA-based skeletal muscle index (SMI) measurement as the primary screening tool for sarcopenia in Asian populations. Specifically, the AWGS threshold is SMI < 7.0 kg/m² in men and < 5.4 kg/m² in women. InBody BIA directly calculates SMI from segmental lean analysis data and displays it on the result sheet relative to these thresholds. As a result, sarcopenia screening that previously required specialist referral can now be integrated into routine geriatric outpatient assessment in under 60 seconds.
Oncology Nutritional Support
In oncology, skeletal muscle mass is a direct predictor of chemotherapy tolerance, surgical outcomes, and overall survival. Moreover, the ECW/TBW ratio tracks the inflammatory and oedematous changes that accompany cancer treatment and nutritional depletion. Therefore, InBody BIA serial monitoring allows oncology nutrition teams to intervene early when muscle wasting or fluid dysregulation is detected before it reaches the threshold of clinical cachexia.
How to Prepare for an InBody BIA Scan: Clinical Protocols
BIA is sensitive to hydration status and recent food intake. Consequently, following a standardised preparation protocol ensures that results are reproducible and comparable across serial scans.
- Fast for at least 2 hours before scanning. Recent food and fluid intake alters body water distribution, affecting impedance readings. For research-grade consistency, a 4-hour fast is preferred.
- Avoid intense exercise for 12 hours before scanning. Vigorous exercise causes temporary fluid shifts into muscle tissue, transiently elevating lean mass readings.
- Avoid alcohol for 24 hours before scanning. Alcohol is a diuretic. It alters total body water and ECW/TBW distribution independently of actual body composition.
- Scan at the same time of day for serial comparisons. Body water shifts diurnally, typically 0.5–1.5 kg between morning and evening. Scanning at a consistent time removes this source of variability.
- Remove all metal jewellery and accessories. Metal objects can interfere with electrode contact and impedance measurement.
- For women, avoid scanning during the premenstrual week. Hormonal fluid retention in this phase can transiently elevate extracellular water and body weight readings.
CONTRAINDICATIONS
InBody BIA is contraindicated in patients with implanted electronic devices, specifically pacemakers and implantable cardioverter-defibrillators (ICDs). The electrical current, while safe for healthy tissue, can theoretically interfere with device function. Additionally, BIA is not recommended during pregnancy due to the absence of validated reference ranges for pregnant patients. For all other patient groups, including elderly, paediatric, and post-surgical patients. InBody BIA is safe, non-invasive, and radiation-free.
Frequently Asked Questions
InBody DSM‑BIA demonstrates 98.4% accuracy compared with DEXA, while offering better repeatability for serial monitoring and additional clinical metrics like ECW/TBW ratio and segmental lean analysis that DEXA does not provide.
InBody DSM-BIA measures trunk impedance at multiple frequencies, enabling a validated 1–20 visceral fat level estimate that correlates with CT-based visceral fat measurements, making it a practical tool for routine clinical screening.
Body composition scans are typically recommended every 8–12 weeks for general health monitoring, monthly for post-surgery or oncology nutrition tracking, and every 4–6 weeks for elite athletes to monitor training-related changes.
InBody offers multiple models for different needs: InBody 270/380 for basic fitness screening, 570 for clinical nutrition with ECW/TBW analysis, 770 for hospital use with android–gynoid ratio, and 970 for advanced research with detailed segmental data and phase angle. 📊
One-line rephrased version:
InBody DSM-BIA calculates body composition directly from measured impedance and physical constants—without using population-based equations—allowing accurate results across diverse body types such as thin-fat individuals, athletes, elderly patients, and post-surgical cases.
Key Takeaways for Medical Practitioners
- BIA measures body composition by quantifying the electrical impedance, the resistance, and reactance of body tissues to a safe electrical current.
- InBody’s DSM-BIA measures five body segments independently at up to six frequencies, eliminating the single-cylinder assumptions and empirical equations that limit traditional BIA accuracy.
- InBody achieves 98.4% accuracy vs DEXA with no radiation, in under 60 seconds, at a fraction of DEXA’s cost, making it the practical standard for routine body composition monitoring.
- Eight key markers, body fat %, skeletal muscle mass, visceral fat level, ECW/TBW ratio, segmental lean analysis, trunk fat, android/gynoid ratio, and InBody Score, provide a complete metabolic risk picture.
- InBody is especially critical for Indian patients because it uses direct impedance measurement rather than Western population equations and applies Asian-specific reference ranges.
- Clinical applications span diabetes care, bariatric surgery, sports medicine, geriatric sarcopenia screening, and oncology nutrition, all contexts where body composition changes are clinically significant but invisible to BMI or standard blood tests.
Bring Clinical-Grade Body Composition Analysis to Your Practice
An InBody scan provides the tissue-level data your patients need for truly personalised, evidence-based clinical management in under 60 seconds, with no radiation and no specialist requirement.
Find an InBody Scanner Near You
References & Clinical Sources
- InBody Co. “Validation of InBody BIA against DEXA in diverse clinical populations.” InBody White Paper Series. Seoul: InBody Co., 2022.
- Yajnik CS, Yudkin JS. “The Y-Y paradox.” The Lancet. 2004;363(9403):163.
- WHO Expert Consultation. “Appropriate body-mass index for Asian populations.” The Lancet. 2004;363(9403):157–163.
- DeFronzo RA, et al. “Skeletal muscle insulin resistance is the primary defect in type 2 diabetes.” Diabetes Care. 2009.
- Asian Working Group for Sarcopenia. “2019 Consensus Update on Sarcopenia.” JAMDA. 2020.
- Misra A, et al. “Consensus statement for diagnosis of obesity for Asian Indians.” JAPI. 2009.
- International Diabetes Federation. IDF Diabetes Atlas, 10th Edition. Brussels: IDF, 2021.
- Neeland IJ, et al. “Visceral and ectopic fat, atherosclerosis, and cardiometabolic disease.” Obesity Reviews. 2019.
- Kim TN, Choi KM. “Sarcopenia: Definition, epidemiology, and pathophysiology.” Journal of Bone Metabolism. 2013.
- Roth J, et al. “Muscle-fat interactions — immunological mechanisms and clinical implications.” Frontiers in Immunology. 2021.

Most trending articles

InBody vs DEXA vs Skinfold Calipers: Which Body Composition Test Is Right for You in India?
DEXA scans, InBody BIA, skinfold calipers — three different ways to measure body composition. Accuracy comparisons, cost in India, accessibility, and which method makes sense for your specific goal.

Skinny Fat in India: Why 40% of Normal Weight Indians Have Dangerously High Body Fat
India's hidden obesity epidemic. Skinny fat (TOFI — Thin Outside, Fat Inside) affects millions of normal-weight Indians. How body composition testing reveals what BMI hides — and the exact protocol to fix it.

Healthy Body Composition by Age for Indians: Reference Ranges at 20s, 30s, 40s, 50s+
Body composition reference ranges for Indian men and women by age. Find out if your body fat %, muscle mass, and visceral fat level are healthy for your age and what to do if they're not.