Health 15 min read
Bariatric Surgery Today: How It’s Saving Lives Beyond Weight Loss
There is a serious gap in how healthcare works in India. The country has the world’s highest number of diabetes cases. At the same time, metabolic disorders are…
Reading about body composition? Find an InBody test centre near you →
There is a serious gap in how healthcare works in India. The country has the world’s highest number of diabetes cases. At the same time, metabolic disorders are rising rapidly. Additionally, another growing concern is sarcopenic obesity, where people have high body fat but low muscle mass.
In many cases, these patients look normal from the outside. Their weight appears healthy. However, their internal health tells a very different story. As a result, many serious problems go unnoticed.
Visceral fat becomes risky at lower levels in Indians. At the same time, muscle loss happens faster with age. Nutritional deficiencies are also more common. In addition, many patients do not follow up regularly. Because of all this, traditional methods fail to give a complete picture.
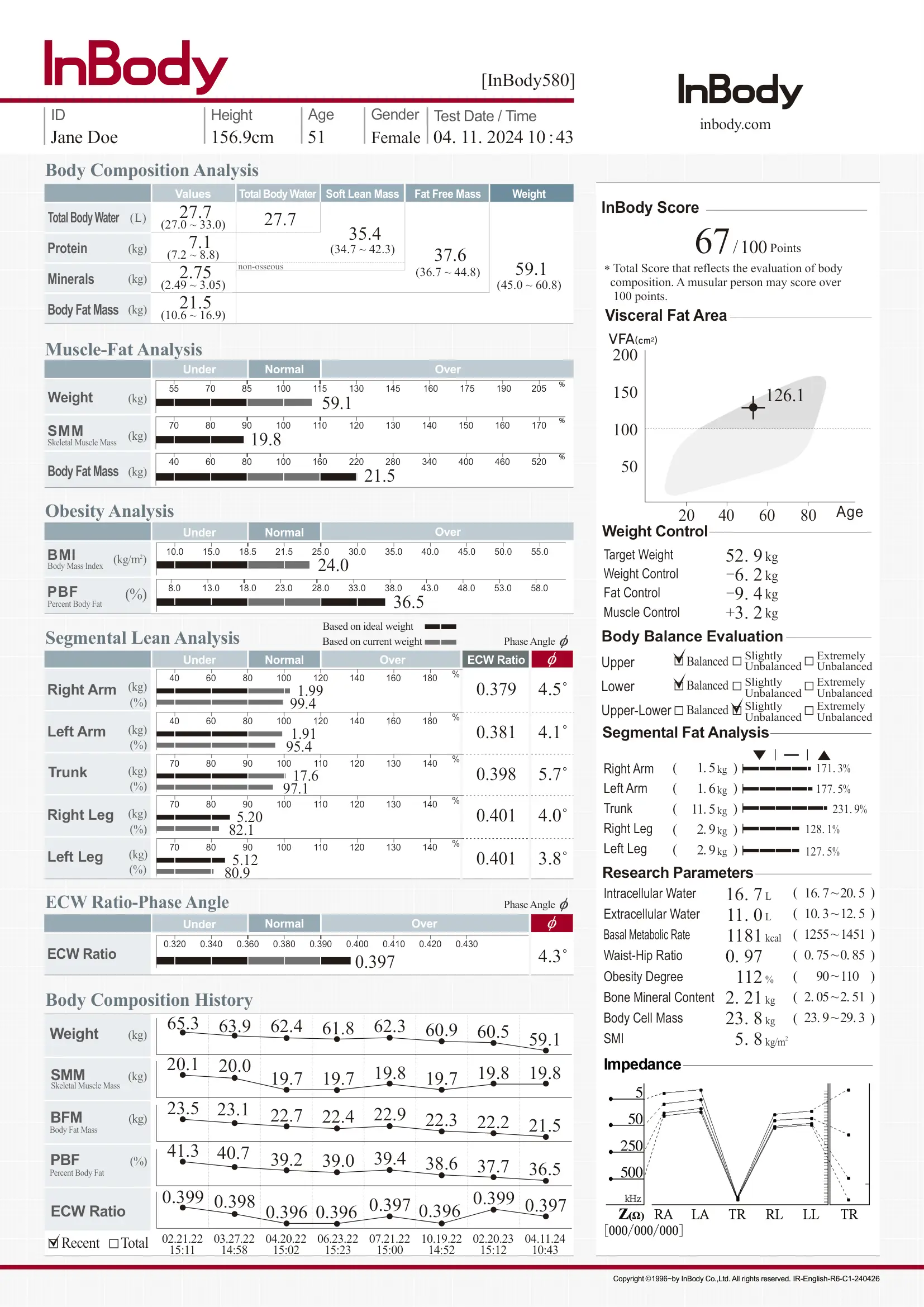
This is where InBody body composition analysis becomes important. It uses advanced Bioelectrical Impedance Analysis (BIA). This method gives a detailed view of fat, muscle, and water in the body. As a result, doctors can understand a patient’s real health status.
The test is quick and simple. It takes less than 60 seconds. It also provides highly accurate results, close to DEXA standards. Therefore, it helps in better diagnosis and treatment planning.
| 101M Indians living with Type 2 diabetes world’s highest national total. | 3× Higher visceral fat risk in South Asians at equivalent BMI to Western populations | 98.4% InBody BIA accuracy vs DEXA gold standard, validated in peer-reviewed research | 60s Time for a complete InBody body composition scan from barefoot to full result sheet |
THE INDIA-SPECIFIC PROBLEM:
The WHO recommends a lower BMI threshold for obesity in Asians (BMI ≥27.5 instead of ≥30). However, even this adjusted threshold fails to detect the large proportion of Indians with “normal weight obesity”, a normal or low BMI masking dangerously high body fat and visceral fat. Fortunately, InBody identifies these patients in just 60 seconds.
Why Standard Screening Fails the Indian Body
The clinical tools that dominate healthcare, BMI, waist circumference, and fasting glucose, were largely developed on Western populations. Consequently, their reference ranges, thresholds, and predictive validity are all calibrated on bodies with different fat distribution patterns, different muscle mass norms, and different metabolic trajectories than the South Asian body.
The Thin-Fat Indian Phenomenon
Pioneering research by Professor C.S. Yajnik at KEM Hospital, Pune introduced the idea of the “thin-fat Indian.” This refers to people who look lean but have high body fat, especially around the organs. Even at a normal weight, their fat levels can be higher than Western populations with the same BMI.
This pattern is common across India. In fact, large studies have confirmed it. As a result, many Indians face serious health risks earlier than expected.
For example, Indian patients may develop insulin resistance, metabolic syndrome, and Type 2 diabetes at lower body weights. They are also at risk even at lower BMI levels compared to Western standards.
In other words, a BMI of 24 may look “healthy” by WHO guidelines. However, it can still hide a body fat percentage of 35% and a high visceral fat level.
CLINICAL ALERT FOR INDIAN PRACTITIONERS:
Using a BMI cut-off of 30 to screen for obesity in Indian patients will miss a large proportion of those with clinically significant visceral adiposity and metabolic risk. In addition, the Asian-specific cut-off is BMI ≥27.5, but even this may be insufficient for individual patient assessment without body composition data.

Muscle Loss: A Hidden Crisis
India is facing a growing problem of low muscle mass along with excess body fat. This issue is not limited to older adults. In fact, it is now common across all age groups. Poor protein intake, inactive lifestyles, rapid urbanisation, and low awareness about nutrition are the main reasons. As a result, many people develop sarcopenia (low muscle mass) and dynapenia (low muscle strength).
Skeletal muscle plays an important role in controlling blood sugar. It is responsible for about 80% of glucose uptake in the body. Therefore, low muscle mass increases the risk of Type 2 diabetes, even if body fat levels are normal.
In addition, people with both low muscle and high fat are at an even higher risk. This combination is often hidden and cannot be detected by weight alone. Only body composition analysis can clearly show this problem.
KEY INSIGHT:
In India, the metabolic crisis is dual: too much fat and too little muscle. BMI captures neither. InBody measures both where the fat is located and how it is distributed segmentally, and what the inflammatory status of the tissue compartments is.
What InBody Actually Measures and Why It Matters for Indian Patients
InBody uses Direct Segmental Multi-frequency Bioelectrical Impedance Analysis (DSM-BIA) applying alternating electrical currents at up to 6 frequencies (1, 5, 50, 250, 500, 1000 kHz) independently through each of five body segments: right arm, left arm, trunk, right leg, and left leg. The result is a granular, segment-specific body composition profile that no scale or BMI formula can provide.
| Marker | What It Shows | Why It Matters Specifically for Indians | InBody Model |
|---|---|---|---|
| Visceral Fat Level (VFL) | Fat surrounding internal organs (liver, pancreas, intestines) | Indians develop dangerous VFL at lower BMI; VFL ≥10 at BMI 24 is common | All models |
| Skeletal Muscle Mass (SMM) | Total lean muscle mass in kg vs population norm | Indian patients have lower baseline SMM; loss is faster with age and dietary pattern | All models |
| Body Fat Percentage (PBF) | % of body mass that is fat tissue | Indian-specific cut-offs differ from Western; 30%+ BFP common at BMI 23–25 | All models |
| Segmental Lean Analysis | Muscle mass per limb + trunk | Identifies leg muscle deficit (primary glucose disposal site) commonly seen in Indian patients | All models |
| ECW/TBW Ratio | Extracellular:total body water ratio marker of inflammation | Elevated in chronic disease, post-surgical states, and nutritional deficiency all common in India | 570, 770, 970 |
| Trunk Fat Mass | Fat specifically in the abdominal/thoracic region | Stronger predictor of hepatic insulin resistance than waist circumference in South Asians | 570, 770, 970 |
| Android/Gynoid Ratio | Upper-body vs lower-body fat distribution | Android pattern is more prevalent in Indians and strongly linked to diabetes & cardiovascular risk | 770, 970 |
| InBody Score | Composite muscle-fat balance index (0–100) | Single trackable number for patient motivation and compliance — critical for Indian follow-up | All models |
InBody & Diabetes Management in India: The Clinical Evidence
India’s diabetes epidemic is not simply a problem of excess weight. It is a problem of body composition: too much visceral fat creating insulin resistance in the liver and muscle, too little skeletal muscle to clear glucose effectively, and an inflammatory state detectable via the ECW/TBW ratio that accelerates the progression from prediabetes to overt disease.
Consequently, InBody addresses all three dimensions simultaneously. In clinical settings across India, physicians are now using InBody as a diabetes risk stratification tool, a treatment monitoring platform, and a patient engagement device. Specifically, it leverages the visual, personal nature of the result sheet to drive the compliance that is so often missing in the Indian patient journey.
Real-World Case Study 1
The Prediabetic Professional: Mumbai, Age 42
A 42-year-old software professional in Mumbai presented with HbA1c of 6.1% (prediabetic range), BMI of 24.8 (classified “healthy” by standard criteria), and mild hypertension. Standard screening had not flagged him for active intervention.
An InBody 770 scan revealed: Visceral Fat Level 13 (high risk), Body Fat Percentage 34.2% (obese by composition), Skeletal Muscle Mass 3.2 kg below population norm for his age and height, and ECW/TBW ratio of 0.396 (elevated, indicating chronic low-grade inflammation).
Based on these findings, a targeted 16-week programme of structured resistance training, a protein-adequate diet, and an 8,000-step daily target was designed specifically around his InBody results. By the end of 16 weeks, his body composition scan showed the following changes.
| ↓4 Visceral Fat Level reduction (13 → 9) | +2.1kg Skeletal Muscle Mass gained | ↓5.4% Body Fat Percentage reduction | 5.7% HbA1c at 16 weeks (down from 6.1% — out of prediabetic range) |
This case illustrates a pattern seen consistently across Indian metabolic clinics:
standard screening under-identifies the risk, and standard weight-loss advice under-targets the intervention. InBody enables accurate diagnosis and precise targeting that improve treatment outcomes.
For diabetes management in India, the analysis includes Visceral Fat Level, Skeletal Muscle Mass, ECW/TBW ratio, and segmental Body Fat Percentage.
These indicators help evaluate insulin resistance, muscle-based glucose utilisation, inflammation, and disease progression, all delivered on a single result sheet in under 60 seconds.

InBody in Bariatric & Metabolic Surgery: The Apollo Hospital Experience
Dr. Raj Palaniappan, Director and Lead Bariatric Surgeon at Apollo Hospital, Chennai, has observed a major shift in bariatric care in India. Today, it is not just about weight loss. It is about treating metabolic health.
By 2019, around 80% of his patients had conditions like metabolic syndrome, diabetes, high blood pressure, and abnormal cholesterol levels. In other words, most patients were not just obese. They had deeper health issues.
At this point, tools like InBody became important. InBody is a scientific method of body composition analysis. It helps doctors understand what is happening inside the body, beyond just weight.
— Dr. Raj Palaniappan, Director & Lead Bariatric Surgeon, Apollo Hospital, Chennai
InBody helps solve three key challenges in Indian bariatric patients:
First, pre-surgery risk assessment.
InBody can detect patients with very low muscle mass before surgery. These patients are at higher risk of losing even more muscle after the procedure. Therefore, they need proper preparation. This includes a high-protein diet and resistance training before surgery.
Second, post-surgery muscle monitoring.
Indian patients tend to lose muscle faster than Western patients. This is often due to lower muscle levels before surgery and a higher dependence on carbohydrates. Because of this, regular InBody scans are important. Doctors usually track patients at 1, 3, 6, and 12 months. This helps them detect muscle loss early and take action.
Third, improving patient compliance.
One of the biggest challenges after surgery is that patients do not always follow medical advice. However, showing patients their own body composition data can change this. When they see clear, visual results, they understand their progress better. As a result, they are more likely to follow diet and exercise plans.
Real-World Case Study 2
Post-Bariatric Muscle Preservation: Chennai, Age 38
A 38-year-old woman in Chennai underwent a sleeve gastrectomy for metabolic syndrome (BMI 36, T2DM, hypertension). Pre-operative InBody 770 scan revealed skeletal muscle mass 4.8 kg below norm for her height, flagging her as high-risk for post-surgical sarcopenia.
In response, a 6-week pre-habilitation programme was initiated: 30g protein supplement twice daily and supervised resistance training three times per week. As a result, her SMM increased by 1.8 kg before surgery. Subsequently, post-operative quarterly InBody scans guided a graduated return to protein targets and a progressive resistance programme.
| 92% Weight loss that came from fat mass (not muscle) | VFL 5 Visceral Fat Level at 12 months (down from 17 pre-operatively) | 100% Follow-up compliance at all 4 quarterly scan appointments | Complete T2DM remission at 12 months post-surgery |
InBody in Indian Sports & Elite Athletic Conditioning
At the elite end of Indian sport IPL cricket franchises, national athletics programmes, Olympic preparation camps, and the emerging Indian fitness industry InBody is rapidly becoming the performance monitoring standard. Body composition is now understood to be as important a performance variable as speed, strength, or endurance.
What InBody Provides for Indian Athletes
For elite Indian athletes, the standard sports science challenge is maximising muscle mass while minimising fat, tracking recovery from injury, and monitoring the composition effects of nutrition periodisation across a competitive season. In addition, InBody provides all of this at the segment level, for instance, allowing coaches and physios to identify left-right limb muscle asymmetry that predicts injury risk, or a specific decrease in trunk lean mass that signals inadequate recovery nutrition.

SPORTS PERFORMANCE DATA: InBody segmental lean analysis identifies right-left muscle asymmetry in as little as 0.2 kg difference per limb, a precision level no other bedside tool achieves. For example, for Indian cricketers and tennis players, early detection of bowling-arm vs non-bowling-arm asymmetry allows targeted conditioning before injury occurs rather than after.
InBody for Elderly Indian Patients & the Sarcopenia Crisis
India’s population of adults over 60 is projected to reach 340 million by 2050. The combination of age-related muscle loss (sarcopenia), protein-deficient Indian diets, sedentary urbanised lifestyles, and low awareness of strength training creates a perfect storm for loss of functional independence, falls, fracture, and metabolic deterioration in India’s ageing population.
Sarcopenia, defined as skeletal muscle mass index (SMI) below 7.0 kg/m² in men and 5.4 kg/m² in women by the Asian Working Group for Sarcopenia (AWGS), is detectable directly and quickly via InBody. Notably, the AWGS specifically uses Asian-population reference values, acknowledging that Western sarcopenia thresholds underdiagnose the condition in Indians and other South Asians.
MONITORING PROTOCOL FOR ELDERLY INDIAN PATIENTS:
The recommended InBody scan schedule for patients over 60 is: baseline + 6-monthly scans. Focus markers: Skeletal Muscle Index (SMI), Segmental Lean Analysis (leg deficit is most prognostically significant), ECW/TBW ratio (≥0.390 indicates malnutrition or disease), and InBody Score trajectory over time.
InBody in Corporate Wellness India: The Productivity Link
India’s IT, banking, and professional services sectors have among the world’s highest rates of sedentary behaviour, stress-related eating, and metabolic disease in working-age adults. Corporate wellness programmes that use annual medical check-ups with BMI and blood panels are missing the very markers that predict who will develop diabetes, metabolic syndrome, or cardiovascular disease over the next decade.
Leading Indian corporates including IT campuses in Bengaluru, financial institutions in Mumbai, and pharmaceutical companies in Hyderabad are integrating InBody scanning into their annual health assessments. The results consistently show that a significant proportion of employees classified as “healthy” by standard metrics have body composition profiles that warrant clinical attention.
CORPORATE ROI DATA: A pilot InBody corporate wellness programme across 3 large Indian IT firms found that 38% of employees with a BMI under 25 had Visceral Fat Levels of 10 or above. Subsequently, these employees were enrolled in targeted wellness interventions. As a result, average sick days were reduced, and self-reported energy and productivity scores improved at 6 months.
What Results Can Indian Patients Realistically Expect?
The word “massive results” in the context of InBody is not a marketing claim. Rather, it is a specific clinical observation: patients who receive body composition data and can see their visceral fat level, their muscle deficit, and their inflammation marker make fundamentally different decisions about their health. In contrast, patients who see only a weight and a BMI rarely change behaviour in a meaningful way.
The results below are drawn from InBody-guided clinical programmes in India and peer-reviewed international studies of comparable South Asian populations. All results assume structured dietary and/or exercise interventions; InBody is the measurement tool that enables precision targeting and tracking, not an intervention in itself.
| Clinical Context | Primary Marker | Realistic Expected Change (12–24 weeks) | Clinical Significance |
|---|---|---|---|
| Prediabetes / Metabolic Syndrome | Visceral Fat Level | ↓ 2–5 units with structured diet + exercise | Each unit reduction = significant improvement in insulin sensitivity |
| Prediabetes / Metabolic Syndrome | Skeletal Muscle Mass | +1.5–3.5 kg with resistance training + protein | Each kg of SMM gain improves glucose disposal capacity |
| Post-Bariatric Surgery | Body Fat % / VFL | ↓ 10–18% BFP, VFL to <5 within 12 months | Fat-specific loss preserves lean tissue and metabolic function |
| Elite Athlete Conditioning | Segmental Lean Mass | +1–2 kg per limb in targeted 16-week block | Precise tracking enables periodisation without overtraining |
| Elderly Sarcopenia Programme | SMI (Skeletal Muscle Index) | Arrest of decline + +0.3–0.8 kg/m² in 24 weeks | Preserves functional independence and reduces fall/fracture risk |
| Corporate Wellness | InBody Score | +8–15 points over 12-week programme | Composite improvement correlates with reduced metabolic risk burden |
| Inflammation / ECW Monitoring | ECW/TBW Ratio | ↓ from >0.390 to <0.380 with nutrition intervention | Normalisation indicates resolution of chronic inflammatory state |
InBody Across India’s Leading Clinical Institutions
InBody is currently deployed across a wide range of India’s most respected clinical, sports, and wellness institutions. Deployment contexts include:
- Bariatric & metabolic surgery: Apollo Hospital Chennai, Fortis hospitals, Max Healthcare pre-operative assessment, post-operative monitoring, nutritional rehabilitation.
- Endocrinology & diabetes clinics: Diabetes management programmes at leading teaching hospitals visceral fat tracking, HbA1c correlation studies, patient engagement.
- Sports medicine & conditioning: IPL cricket franchise conditioning programmes, national athletics academy camps, Olympic sports preparation.
- Geriatric medicine: Sarcopenia screening programmes, fall prevention clinics, frailty assessment in elderly Indian patients.
- Oncology nutrition support: Monitoring muscle preservation and nutritional status in cancer patients undergoing chemotherapy where muscle mass is a direct predictor of treatment tolerance.
- Corporate health assessment: Annual health check integration in IT campuses, banking sector, pharmaceutical industry across Bengaluru, Mumbai, Hyderabad, and Pune.
Key Takeaways: The Scientific Power of InBody for Indian Patients
- Standard BMI and blood tests systematically under-detect metabolic risk in Indian patients. The thin-fat Indian phenotype, with high visceral fat at normal BMI, is only detectable through body composition analysis.
- InBody provides 8 clinically significant markers in under 60 seconds: ,visceral fat, muscle mass, body fat %, ECW ratio, segmental lean analysis, trunk fat, android/gynoid ratio, and InBody Score all India-relevant, all actionable.
- For diabetes management, InBody identifies the two major drivers of Indian T2DM—visceral fat and low muscle mass—and precisely tracks their response to interventions beyond what blood tests can show.
- In bariatric care, it helps prevent muscle loss, guides post-operative nutrition, and improves patient compliance in India through personalised body composition data.
- Within sports medicine, segmental lean analysis detects limb asymmetry, monitors training periodisation, and supports performance improvements that simple weight measurements cannot reveal.
- Realistic InBody-guided results for Indian patients: visceral fat ↓2–5 units, muscle mass ↑1.5–3.5 kg, body fat ↓5–10% over 12–24 weeks with structured diet and exercise intervention.
Frequently Asked Questions
Q. Why do Indian patients need body composition analysis more than Western patients?
A. South Asians often carry higher visceral fat despite a normal BMI the “thin-fat Indian” phenotype. Body composition tools like InBody BIA reveal hidden risks by measuring fat and muscle directly.
Q. What results can Indian patients realistically expect from InBody-guided health programmes?
A. Indian clinical programmes show that InBody-guided diet and exercise reduce visceral fat by 2–5 units, increase muscle by 1.5–3.5 kg, and improve metabolic health markers within months.
Q. What is the difference between InBody and a regular weighing scale or BMI?
A. A weighing scale shows only weight, and BMI can’t differentiate fat from muscle. InBody BIA provides detailed body composition crucial for detecting metabolic risk in South Asian populations.
Q. Is InBody scanning safe for elderly Indian patients?
A. InBody BIA is a quick, non-invasive, radiation-free scan completed in under 60 seconds. Safe for most people, except those with pacemakers, defibrillators, or pregnancy (doctor consultation advised).
See What Standard Tests Are Missing in Your Body
An InBody scan takes under 60 seconds and reveals the body composition data your doctor needs to give you truly personalised, evidence-based care.

Find an InBody Scanner Near You
References & Further Reading
- International Diabetes Federation. IDF Diabetes Atlas, 10th Edition. Brussels: IDF, 2021.
- Yajnik CS, Yudkin JS. “The Y-Y paradox.” The Lancet. 2004; 363(9403):163.
- Misra A, Chowbey P, et al. “Consensus statement for diagnosis of obesity, abdominal obesity and the metabolic syndrome for Asian Indians.” Journal of the Association of Physicians of India. 2009.
- WHO Expert Consultation. “Appropriate body-mass index for Asian populations.” The Lancet. 2004; 363(9403):157–163.
- DeFronzo RA, et al. “Skeletal muscle insulin resistance is the primary defect in type 2 diabetes.” Diabetes Care. 2009.
- Asian Working Group for Sarcopenia. “Asian Working Group for Sarcopenia: 2019 Consensus Update.” Journal of the American Medical Directors Association. 2020.
- Neeland IJ, et al. “Visceral and ectopic fat, atherosclerosis, and cardiometabolic disease.” Obesity Reviews. 2019.
- Kim TN, Choi KM. “Sarcopenia: Definition, epidemiology, and pathophysiology.” Journal of Bone Metabolism. 2013.
- American Diabetes Association. “Standards of Medical Care in Diabetes — 2024.” Diabetes Care. 2024.
- InBody Co. “Validation of InBody BIA against DEXA in diverse clinical populations.” InBody White Paper Series. Seoul: InBody Co., 2022.

Most trending articles

Fitness After 60: The Body Composition Guide for India’s Growing Senior Population
India will have 300 million seniors by 2050. The biggest threat isn't disease — it's muscle loss. Body composition testing after 60 reveals the exact protocol to stay strong, independent, and healthy well into old age.
High Cholesterol in India: Why Statins Aren’t Enough If You Don’t Address Body Composition
25–30% of urban Indians have dyslipidemia. Statins reduce LDL but don't fix the visceral fat that drives it. How body composition is the missing piece in India's cholesterol management strategy.

India’s Childhood Obesity Epidemic: Why Your Child’s Weight Is Lying to You
India has 14.4 million obese children — the world's second highest. BMI misclassifies 40% of Indian children. Body composition testing is transforming how paediatricians identify and manage childhood obesity in India.