You look slim. Your BMI is normal. But your metabolic health tells a completely different story, and no amount of cardio will fix what you cannot measure.
Key Statistics
| 30–40% Of Indians with normal BMI may have excess body fat (MONW) | 2× Higher cardiovascular risk in skinny fat vs metabolically healthy individuals | 0% Muscle built through cardio alone it needs resistance training | <60s Time for a full InBody body composition scan |
Skinny fat, normal weight, hidden risk
You wear the right size. Your BMI is in the healthy range. You run three times a week. By every visible measure, you look fine. But underneath the surface inside your cells, around your organs, in the ratio of muscle to fat that only a body composition scan can reveal, the story is very different. This is skinny fat. And cardio alone will not fix it.
What is ‘skinny fat’ and what is the clinical term?
The colloquial phrase “skinny fat” describes a body state that medicine calls Metabolically Obese Normal Weight (MONW) or sometimes “normal weight obesity.” It refers to individuals who have a normal BMI (18.5–24.9) or body weight, but carry an abnormal proportion of body fat relative to lean muscle mass.
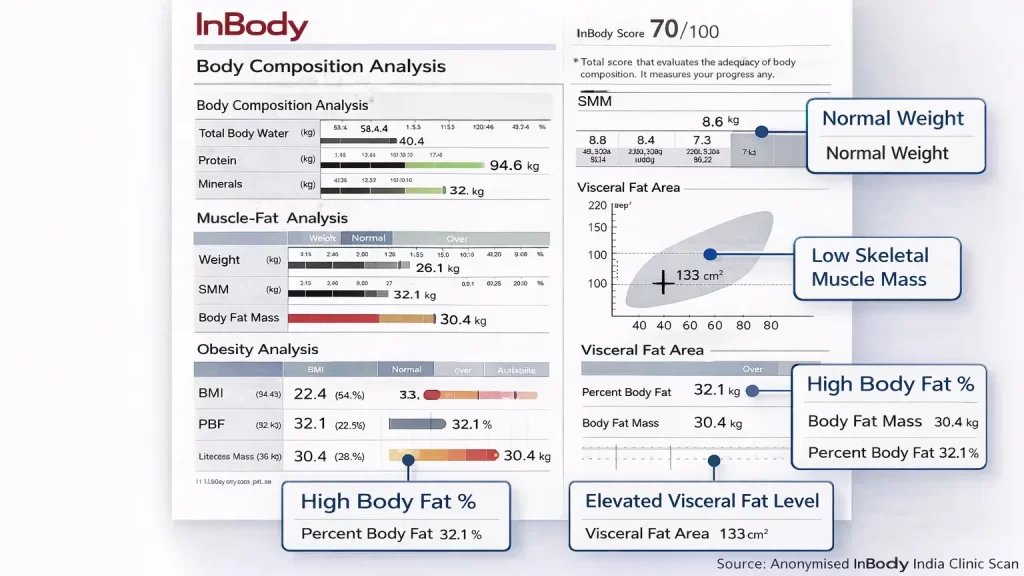
These individuals often look slim or even fit. They may feel healthy. Yet their body composition tells a very different story: high body fat percentage, low skeletal muscle mass, elevated visceral fat, and the cluster of metabolic risks that come with it: insulin resistance, dyslipidaemia, chronic inflammation, and cardiovascular disease risk.
| 30–40% Estimated proportion of normal-weight Indians with metabolic obesity (MONW) | 2× Increased cardiovascular risk in MONW vs metabolically healthy individuals | ~25% Global prevalence of MONW among adults with normal BMI | 101M Indians living with Type 2 diabetes a comorbidity that severely worsens COVID-19 outcomes |
The Indian context: “thin-fat” is especially prevalent in Indian populations, who carry a well-documented genetic predisposition to storing higher proportions of body fat, particularly visceral fat, at lower BMI values compared to Western populations. This “thin-fat Indian” phenotype makes MONW especially common and clinically significant in India, where standard BMI cutoffs may significantly underestimate metabolic risk.
Why BMI and the scale completely miss skinny fat
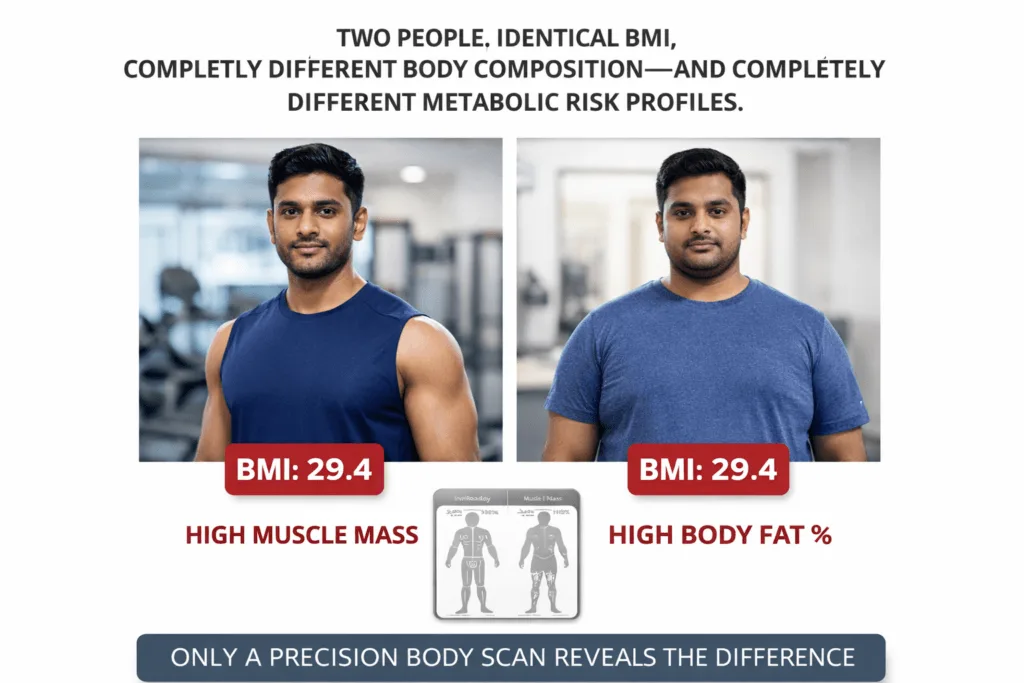
BMI divides body weight by height squared. It knows nothing about what that weight is made of. A person with 35% body fat and very little muscle can have an identical BMI to a person with 18% body fat and strong musculature. On paper, they look the same. Metabolically, they are worlds apart.
Same BMI, very different body composition
The scale has two additional problems for skinny-fat individuals:
- It cannot distinguish fat mass from muscle mass; both register as “weight”
- It cannot locate where fat is stored, visceral fat around organs carries a far higher risk than subcutaneous fat under the skin.
- It cannot detect sarcopenia, insufficient muscle mass masked by a normal weight reading
- Provides no information on cellular health, hydration balance, or metabolic rate.
Key Clinical Insight:
“A normal BMI is not a clean bill of metabolic health. For Indian patients in particular, body composition analysis is the only reliable way to identify MONW because the scale, by definition, cannot see it.”
Why cardio alone cannot fix skinny fat
This is perhaps the most important and least understood principle in skinny fat management. When patients discover they are “skinny fat,” their instinct is to do more cardio. Run more. Cycle more. Walk more. It feels logical: if the problem is too much fat, burn more calories.
But this logic misses the deeper problem. Skinny fat is not simply an excess of fat; it is a deficit of muscle. And cardio does not build muscle.
What cardio actually does to body composition
| Effect | Cardio Only | Resistance Training + Cardio |
|---|---|---|
| Reduces body fat mass | Partially | Yes |
| Builds skeletal muscle mass | No | Yes |
| Improves muscle-to-fat ratio | Minimally | Significantly |
| Increases resting metabolic rate (BMR) | No | Yes |
| Reduces visceral fat | Partially | More effectively |
| Improves insulin sensitivity | Partially | Significantly |
| Prevents lean mass loss during weight loss | No | Yes |
| Improves phase angle (cellular health) | Minimally | Yes |
Cardio can worsen skinny fat. Excessive steady-state cardio without adequate protein intake can trigger muscle catabolism, breaking down the already-insufficient skeletal muscle to fuel exercise. This worsens the muscle-to-fat ratio, lowers BMR further, and deepens the very metabolic problem the patient is trying to solve. InBody serial scans make this visible in real time.
What InBody reveals is that cardio patients never know
For clinicians managing skinny fat or body recomposition patients, InBody body composition analysis provides the only objective picture of what is actually happening inside the body during any intervention, whether cardio, resistance training, diet change, or combined therapy.
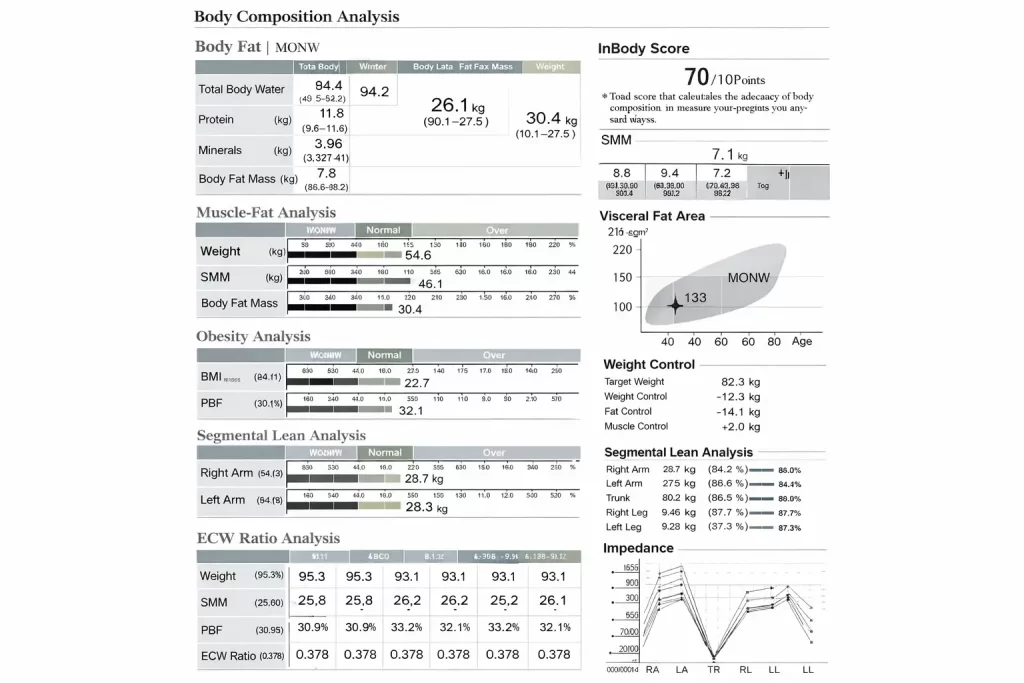
The four InBody parameters most critical in skinny fat assessment:
Skeletal Muscle Mass (SMM) confirms wheth er a muscle deficit is present, the defining marker of skinny fat.
Body Fat Percentage & Mass: Quantifies the hidden fat burden invisible to BMI and scale weight
Visceral Fat Level Measures dangerous organ fat elevated in MONW, even at a normal weight.
Phase Angle reflects cellular integrity and metabolic resilience often low in MONW.
InBody report Skinny fat pattern
What is body recomposition, and why is it the real goal
Body recomposition is the process of simultaneously reducing fat mass and increasing skeletal muscle mass. It is the correct clinical target for skinny fat patients, not simple weight loss, which makes the problem worse by reducing both fat and muscle together.
Why body recomposition is harder to achieve than weight loss:
- It requires building muscle while in a modest caloric deficit or physiologically demanding maintenance
- Requires progressive resistance training, not just cardio or general movement
- It requires adequate protein intake (1.4–2.0 g/kg ideal body weight) to support muscle protein synthesis
- Takes longer than simple weight loss, 12–24 weeks, for meaningful body composition changes
- It cannot be tracked on a standard weighing scale; the weight may stay the same or even increase as muscle is built
Why do body recomposition patients abandon treatment? A patient doing everything right, lifting weights, eating adequate protein, and reducing refined carbohydrates may see no change on the scale for 8–12 weeks. Without InBody data showing fat mass declining and muscle mass rising simultaneously, this patient will conclude the programme is not working and stop. Body composition monitoring is the motivational and clinical anchor for recomposition success.
A clinical protocol for skinny fat management with InBody
The following evidence-informed protocol is recommended for clinicians managing MONW or body recomposition patients:
- Baseline InBody Scan Before Any Intervention: Establish absolute values for SMM, body fat mass, body fat %, visceral fat level, and phase angle. This reveals the true severity of the skinny fat pattern and creates a measurable baseline independent of body weight or BMI
- 2. Classify the Pattern MONW or Sarcopenic Obesity? Use InBody data to determine whether the patient presents as classic MONW (normal weight, high fat, low muscle) or sarcopenic obesity (elevated weight with both high fat and critically low muscle). Management protocols differ.
- Prescribe Resistance Training as the Primary Exercise Intervention, Minimum 3 sessions per week, targeting major muscle groups with progressive overload. This is non-negotiable in skinny fat management. Cardio may be used as a supplement for cardiovascular health and visceral fat reduction, but it must not replace resistance training.
- Optimise Protein Intake Based on InBody FFM Data. Target 1.4–2.0 g/kg of ideal body weight per day, distributed across 3–4 meals. InBody’s fat-free mass data allows precise protein targeting rather than relying on total body weight, which overestimates protein needs in high-fat individuals.
- Monitor Body Composition, Not Body Weight, Every 4–6 Weeks. Repeat InBody scans at 4–6 week intervals to track fat mass loss, SMM gain, visceral fat reduction, and phase angle improvement. Counsel patients that scale weight is an unreliable metric during body recomposition. InBody data is the true progress measure.
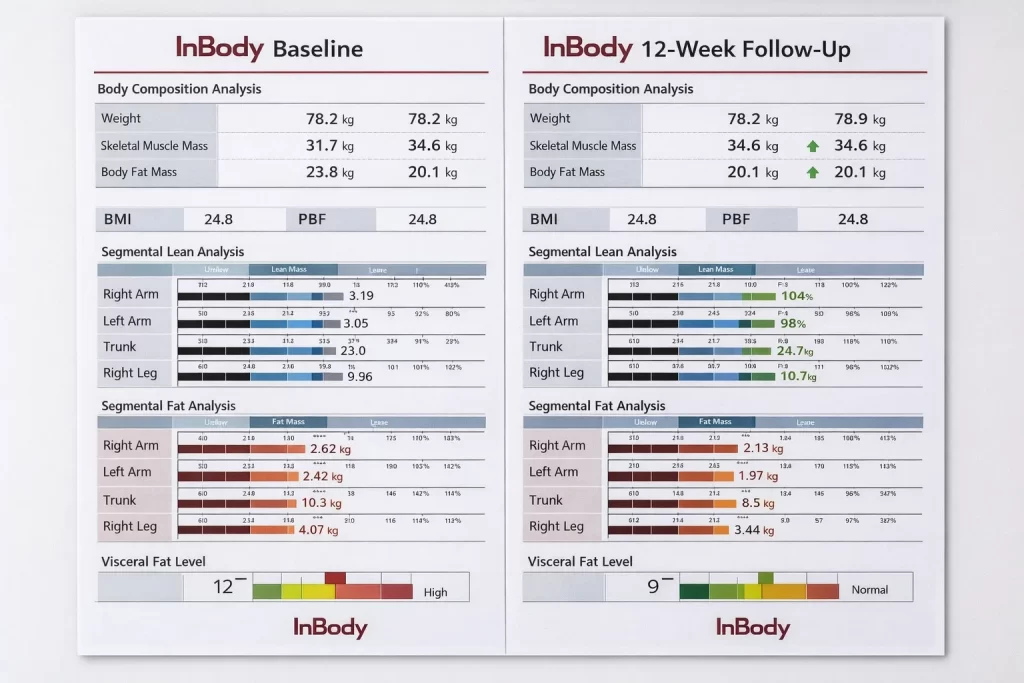
- 12-Week Outcome Review Adjust Strategy: Compare the 12-week InBody report to baseline. Expected positive outcomes: fat mass reduction of 1–3 kg, SMM increase of 0.5–2 kg, visceral fat improvement of 1–3 levels. If progress is inadequate, review exercise compliance, protein intake, sleep quality, and stress levels, all of which affect body recomposition.
InBody-powered body recomposition clinic

MONW and body recomposition represent one of the most underserved patient populations in Indian healthcare. These individuals are typically not diabetic, not obese, and not considered “at risk” by conventional metrics, so they fall through the clinical net. Yet they carry real metabolic risk and are highly motivated to change once given objective data.
For Diabetes & Metabolic Clinics, Skinny-fat patients are pre-diabetic risk cases hiding in a normal-weight population. InBody allows you to identify them, intervene early with body recomposition protocols, and document outcomes objectively, preventing progression to overt type 2 diabetes.
For Fitness & Wellness Clinics, Skinny fat is extremely common among gym-going individuals who do exclusively cardio. InBody data converts frustrated “I exercise, but nothing changes” patients into engaged body recomposition clients because it shows them exactly what is and isn’t working.
For Dietitians & Nutrition Practitioners, protein prescriptions based on total body weight are inaccurate for MONW patients. InBody’s fat-free mass data enables precise, personalised protein targets, and serial scans show whether those targets are supporting muscle retention or growth.
Frequently asked questions
Q. What does ‘skinny fat’ mean medically?
Medically known as Metabolically Obese Normal Weight (MONW), skinny fat describes individuals with a normal BMI or body weight but an unhealthy ratio of fat to muscle. They carry excess body fat, particularly visceral fat, while having insufficient skeletal muscle mass, creating hidden metabolic risk.
Q. Why doesn’t cardio fix skinny fat?
Cardio burns calories and may reduce overall weight, but it does not significantly build skeletal muscle mass. Without increasing muscle, your body composition ratio (fat to muscle) may remain poor or even worsen as cardio can lead to muscle loss alongside fat loss. Resistance training combined with adequate protein is essential for genuine body recomposition.
Q. How does InBody detect skinny fat?
InBody body composition analysers measure skeletal muscle mass, body fat percentage, visceral fat level, and phase angle independently of body weight. A person with a normal BMI can show clearly on an InBody scan that their body fat percentage is high, muscle mass is low, and visceral fat is elevated, the defining pattern of skinny fat.
Q. Is skinny fat common in India?
Yes. Indians have a well-documented genetic predisposition to storing higher body fat at lower BMI values compared to Western populations, a phenomenon sometimes called the ‘thin-fat Indian.’ This makes MONW particularly prevalent and clinically important in the Indian context.
Q. What is body recomposition?
Body recomposition is the process of simultaneously reducing body fat and increasing skeletal muscle mass. Unlike simple weight loss, recomposition improves the quality of your body composition, the ratio of fat to lean tissue, which is the true goal for skinny fat individuals. InBody scans track this process objectively.
Conclusion: the scale is the wrong measuring tool
Skinny fat is a condition defined by what you cannot see and cannot measure with a scale. It lives in the ratio of fat to muscle, in the visceral fat accumulating around organs, in the cellular health markers that decline silently for years before a diagnosis arrives.
Cardio, the default prescription, addresses one part of one dimension of this condition. It burns some calories. It may reduce some fat. But it does nothing to address the muscle deficit at the core of MONW, and in excess, it actively makes that deficit worse.
Real skinny fat transformation requires resistance training, adequate protein, and critically, objective body composition monitoring to know whether the intervention is working. That is what InBody delivers: not a number on a scale, but a complete metabolic picture that guides every clinical decision.
Before and after body recomposition
Ready to offer a skinny fat assessment in your clinic?
InBody body composition analysers give clinicians the data to identify MONW, prescribe precise interventions, and track real recomposition progress beyond what any scale can tell you.

Medical Disclaimer: This blog is intended for healthcare professionals and is for informational and educational purposes only. It does not constitute medical advice, diagnosis, or treatment recommendations. Clinical decisions regarding patient management should be made by qualified healthcare providers based on individual assessment. InBody results should be interpreted in conjunction with a full clinical evaluation.
References & further reading
- Ruderman N, et al. — The Metabolically Obese Normal-Weight Individual Revisited. Diabetes, 1998
- Bhardwaj S, et al. — Prevalence of Metabolic Syndrome Among Indians with Normal BMI. JAPI, 2013
- Yajnik CS, Yudkin JS — The Y-Y Paradox: The Thin-Fat Indian. Lancet, 2004
- Peterson MD, et al. — Resistance Exercise for Muscular Strength in Older Adults. Ageing Research Reviews, 2011
- Thomas DM, et al. — Body Composition and Resting Metabolic Rate. Obesity Reviews, 2012

