Body Composition 8 min read
GLIM Criteria: Why Muscle Mass Beats Albumin in Malnutrition Diagnosis
Albumin: Important but Not Enough – The GLIM Shift Serum albumin is widely used in Indian hospitals and public health programs to assess nutritional status. It helps identify…
Reading about body composition? Find an InBody test centre near you →
Albumin: Important but Not Enough – The GLIM Shift
Serum albumin is widely used in Indian hospitals and public health programs to assess nutritional status. It helps identify patients who may need targeted nutrition therapy, especially in conditions like chronic kidney disease, cancer, or post-surgical recovery.
However, albumin levels can sometimes be misleading. They are often lowered by inflammation, regardless of a person’s actual nutritional reserves. Because of this, albumin is better understood as an inflammation marker (a “negative acute-phase reactant”) rather than a true indicator of nutrition.
Recognising this limitation, four major societies, ASPEN, ESPEN, FELANPE, and PENSA, introduced the Global Leadership Initiative on Malnutrition (GLIM) criteria in 2018. These guidelines emphasise the importance of measuring muscle mass alongside biochemical markers.
Countries like Japan and France already include muscle mass assessment as a regular part of nutrition care. In India, combining muscle mass checks with serum albumin can provide a clearer and more accurate view of a patient’s health.
Ultimately, muscle mass matters. It reflects strength, supports recovery, and gives a better picture of overall health.
What Does GLIM Guidance Mean for Diagnosing Malnutrition?
The Global Leadership Initiative on Malnutrition, better known as GLIM, came into existence in 2016. It was the result of a joint effort between four major international clinical nutrition societies: ESPEN, ASPEN, FELANPE, and PENSA. The goal was simple but ambitious: create a single, worldwide standard for defining and diagnosing malnutrition.
Before this, nutritional assessment often depended on a clinician’s personal judgment. Different countries used different benchmarks, which made research comparisons tricky and slowed down any coordinated global strategy. GLIM was designed to cut through this problem, and over the years, it has caught on. By February 2025, PubMed had listed more than 460 studies referencing the framework.
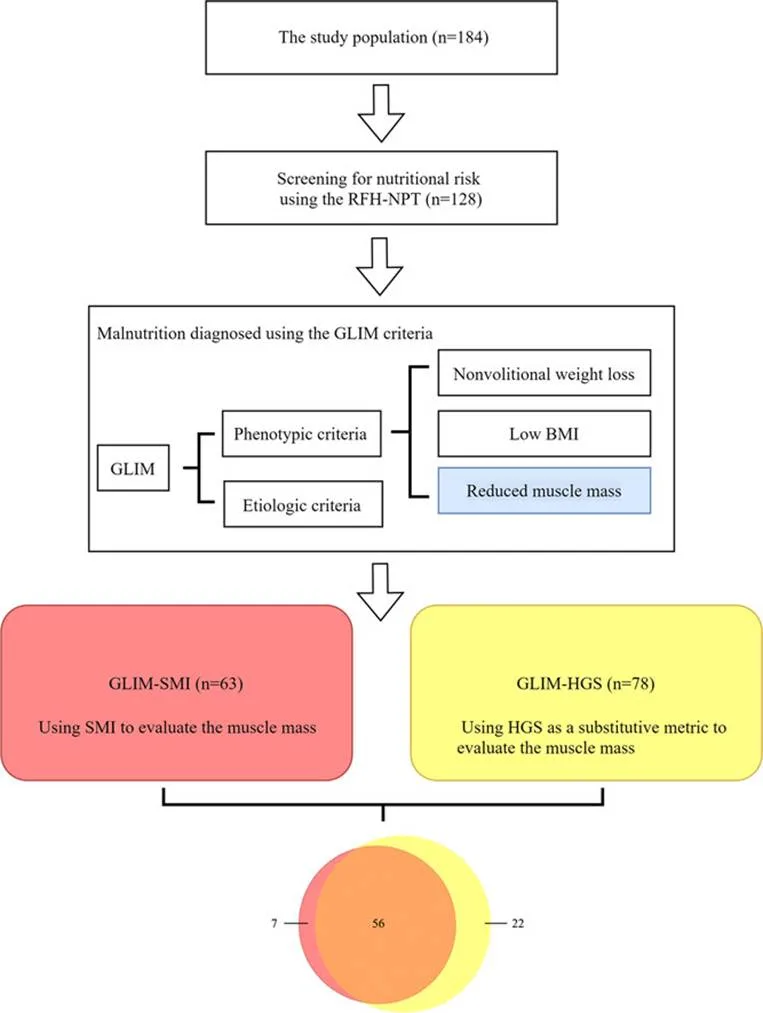
GLIM works in three main stages. First, there’s risk screening, spotting people who might be at risk. This can be done with any validated tool, such as the MUST or NRS-2002. If the person is flagged as “at risk,” the next step is a full diagnostic assessment, which looks at five specific criteria. These are split into two groups: three are phenotypic (relating to body measurements and composition) and two are etiologic (relating to underlying causes). To diagnose malnutrition, you need at least one from each category.
Finally, there’s severity grading, which is based only on the phenotypic measures. This last step is important because it not only confirms the problem but also helps guide how urgently and aggressively it should be treated.
HOW TO USE THE GLIM FRAMEWORK
Why Measuring Muscle Mass Using GLIM Is Often Challenging
When the GLIM criteria were first introduced, they gave a strong overall framework for diagnosing malnutrition. Earlier, there wasn’t much clarity on how to measure muscle mass. It was also unclear what counts as “low muscle mass.”
However, this changed in 2022. New guidelines added more practical details. They did not change the main ideas. Instead, they explained how to measure muscle mass and what numbers to use.
In general, skeletal muscle mass is the best way to assess this. There are a few common methods. These include CT scans, DXA scans, and BIA devices. However, each method works in a different way. So, there is no single standard for everyone.
The cutoffs also vary from person to person. For example, age, sex, and ethnicity all matter. Health conditions can also affect the results.
When it comes to defining “low muscle mass,” experts suggest using existing guidelines. These include sarcopenia guidelines from European and Asian groups. In addition, they borrow ideas from bone health scores like T-scores and Z-scores. This helps keep results consistent.
However, there is one important limitation. None of these tools directly measure muscle. They all estimate it in different ways. Because of this, the results are not always perfect.
For instance, in people with obesity or high body water, results can be misleading. Extra fluid in the body can affect the readings. As a result, muscle mass may look higher than it actually is.
How BWA Technology Fills Gaps in GLIM Muscle Mass Assessment
How InBody Measures Muscle Mass
You see, InBody checks muscle mass using something called Bioelectrical Impedance Analysis (BIA). What’s great about this method is that, unlike CT or DXA scans, it involves no radiation at all. Because of this, it is completely safe, even if you need frequent testing.
The process itself is very simple. A small, harmless electrical signal passes through your body, and you don’t feel anything. As a result, the test is quick and comfortable. In fact, the entire process takes just a few minutes, making it ideal for regularly tracking your nutrition and muscle health.
Why InBody BWA Stands Out
InBody’s Body Water Analyzer (BWA) is a top-tier medical device. Moreover, it is designed to address many of the gaps highlighted in the GLIM guidelines. It provides detailed readings that help healthcare professionals measure muscle mass more accurately. In addition, it helps them set practical and realistic cutoff points for better diagnosis.
Advanced Technology Behind BWA
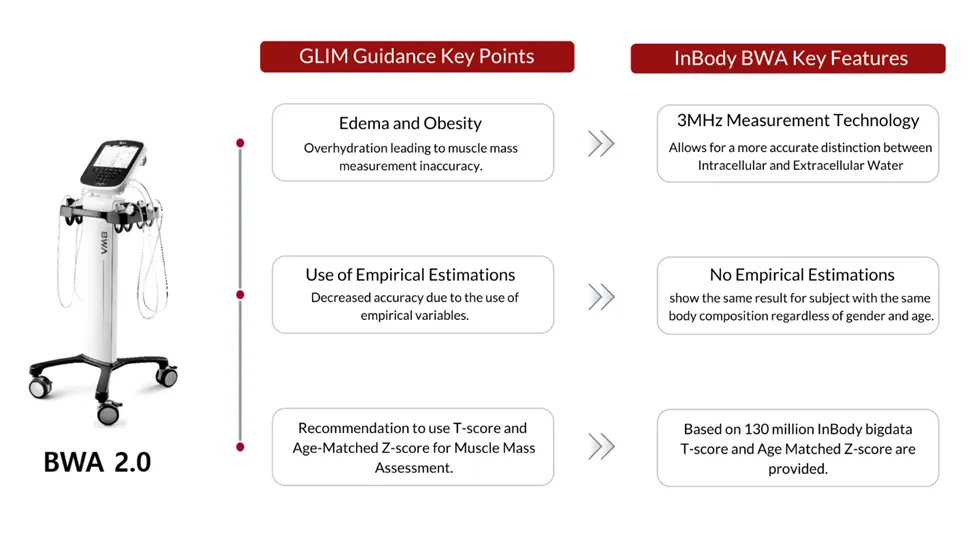
The BWA is the first device in the world to use a 3 MHz high-frequency current. This was once considered difficult to achieve. Because of this advancement, the device can clearly distinguish between extracellular and intracellular water.
Furthermore, it estimates Z₀ and Z∞, which are important values used in both clinical practice and research. As a result, healthcare professionals can better evaluate fluid overload in patients with oedema. At the same time, these insights also improve the accuracy of muscle mass measurements.
How BWA Overcame the Limitations Highlighted in GLIM Guidance
In addition, the BWA provides age-specific assessments based on over 130 million InBody measurements gathered worldwide. These include T-scores, which compare a person’s results to healthy young adults. It also includes age-matched Z-scores, which show how results differ from the average for a specific age group.
Because it focuses on analyzing body fluids, the BWA is especially valuable in key medical areas. These include fluid monitoring, diagnosing sarcopenia, and assessing cellular health.
BWA as a Promising Tool for Sarcopenia Diagnosis
One of the biggest advantages of the BWA is its growing use in diagnosing sarcopenia. It is now being used in both small clinics and large university hospitals.
In 2021, Korea officially recognized sarcopenia as a medical condition. Since then, segmental multi-frequency BIA technology has proven effective in clinical settings. Although it is not yet reimbursed, many doctors are increasingly using InBody devices for regular screening.
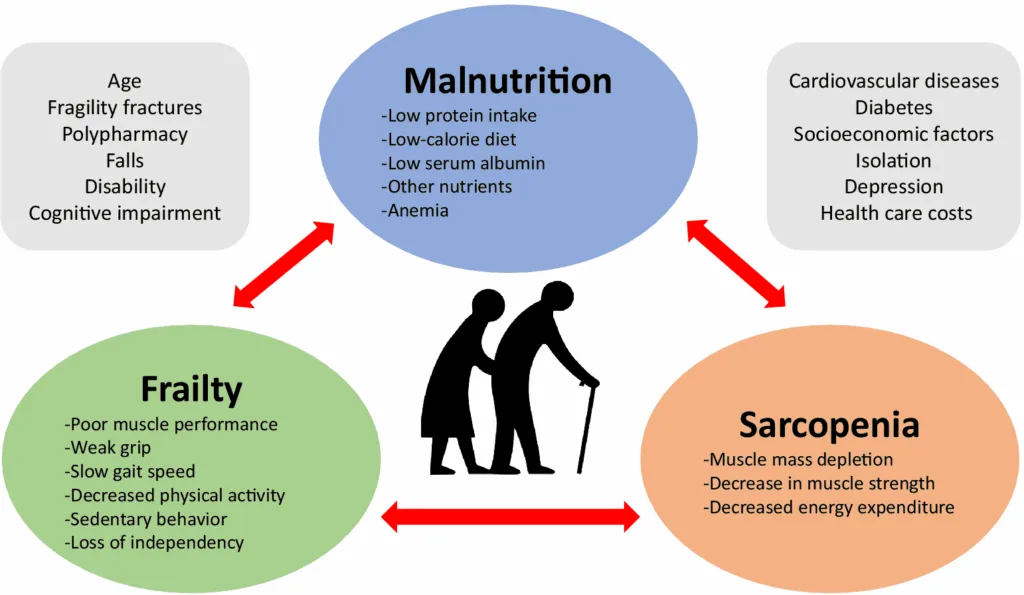
Link Between Sarcopenia and Malnutrition
GLIM guidance also highlights that malnutrition often plays a key role in sarcopenia. Therefore, it recommends closely monitoring nutrition in affected patients.
As this connection becomes clearer, more researchers are turning to BWA for body composition analysis. As a result, it is quickly becoming a trusted tool in both research and clinical practice.
- Muscle mass assessment isn’t just something nice to have anymore it’s actually become a must when it comes to diagnosing malnutrition. Experts everywhere agree on that. Nowadays, since healthcare is focusing more on nutrition, understanding a patient’s muscle condition really matters.
- When doctors have solid, reliable muscle measurements, they can personalize treatments way better. And that often means patients heal and recover faster.
- That’s why it’s so important for clinics and hospitals to keep up with these new developments and use the best ways to check muscle mass methods that are backed by the latest research and guidelines.
Frequently Asked Questions
What are the GLIM criteria for malnutrition?
The Global Leadership Initiative on Malnutrition (GLIM) introduced an approach for malnutrition diagnosis in 2019 comprised of screening followed by assessment of three phenotypic criteria: weight loss, low BMI, and low muscle mass, and two etiologic criteria: reduced food intake/assimilation, and inflammation/disease.
How does malnutrition affect muscle mass?
Interestingly, malnutrition seems to be related to muscle health decline and may contribute to the development of sarcopenia [14,15,16] and aggravate the age-associated loss of muscle mass, muscle strength and physical performance [17,18].
What are the Glim criteria for critical care?
The GLIM criteria for diagnosing malnutrition include three phenotypic criteria: weight loss, low Body Mass Index (BMI), and reduced muscle mass, and two etiologic criteria: reduced food intake or assimilation and chronic and/or acute inflammation.
What are the four indicators of malnutrition?
Common signs and symptoms of malnutrition include:
reduced ability to perform everyday tasks like showering, getting dressed or cooking. Loss of appetite and lack of interest in food or fluids. Unplanned weight loss – this might cause clothing, rings, watches or dentures to become loose.
References
1. Jensen GL, Cederholm T, Ballesteros-Pomar MD, Blaauw R, Isabel M, Cuerda C, et al. Guidance for assessment of the inflammation etiologic criterion for the GLIM diagnosis of malnutrition: A modified Delphi approach. Journal of Parenteral and Enteral Nutrition. 2024 Jan 15;Available from: https://pubmed.ncbi.nlm.nih.gov/38221842/
2. Jensen GL, Cederholm T, Correia MITD, Gonzalez MC, Fukushima R, Higashiguchi T, et al. GLIM Criteria for the Diagnosis of Malnutrition: A Consensus Report From the Global Clinical Nutrition Community. Journal of Parenteral and Enteral Nutrition. 2018 Sep 2;43(1):32–40. Available from: https://pubmed.ncbi.nlm.nih.gov/30181091/
3.Jensen GL, Cederholm T, Correia MITD, Gonzalez MC, Fukushima R, Higashiguchi T, et al. GLIM consensus approach to diagnosis of malnutrition: A 5-year update. JPEN J Parenter Enteral Nutr. 2025;49(1):5–19. Available from: https://aspenjournals.onlinelibrary.wiley.com/doi/10.1002/jpen.2756
4. Compher C, Cederholm T, Correia MITD, Gonzalez MC, Higashiguch T, Shi HP, et al. Guidance for assessment of the muscle mass phenotypic criterion for the Global Leadership Initiative on Malnutrition diagnosis of malnutrition. JPEN Journal of parenteral and enteral nutrition 2022 Apr 19;48(1). Available from: https://pubmed.ncbi.nlm.nih.gov/35437785/
5. Baek JY, Jung HW, Kim KM, Kim M, Park CY, Lee KP, et al. Korean Working Group on Sarcopenia Guideline: Expert Consensus on Sarcopenia Screening and Diagnosis by the Korean Society of Sarcopenia, the Korean Society for Bone and Mineral Research, and the Korean Geriatrics Society. Annals of Geriatric Medicine and Research 2023 27(1):9–21. Available from: https://pubmed.ncbi.nlm.nih.gov/36958807/


Most trending articles

InBody vs DEXA vs Skinfold Calipers: Which Body Composition Test Is Right for You in India?
DEXA scans, InBody BIA, skinfold calipers — three different ways to measure body composition. Accuracy comparisons, cost in India, accessibility, and which method makes sense for your specific goal.

Skinny Fat in India: Why 40% of Normal Weight Indians Have Dangerously High Body Fat
India's hidden obesity epidemic. Skinny fat (TOFI — Thin Outside, Fat Inside) affects millions of normal-weight Indians. How body composition testing reveals what BMI hides — and the exact protocol to fix it.

Healthy Body Composition by Age for Indians: Reference Ranges at 20s, 30s, 40s, 50s+
Body composition reference ranges for Indian men and women by age. Find out if your body fat %, muscle mass, and visceral fat level are healthy for your age and what to do if they're not.