Health 13 min read
What Is Visceral Fat (and Why It’s More Dangerous Than You Think)
Your weighing scale cannot see it. Your BMI cannot find it. But visceral fat is silently working against your health right now. Unlike the fat you can see…
Reading about body composition? Find an InBody test centre near you →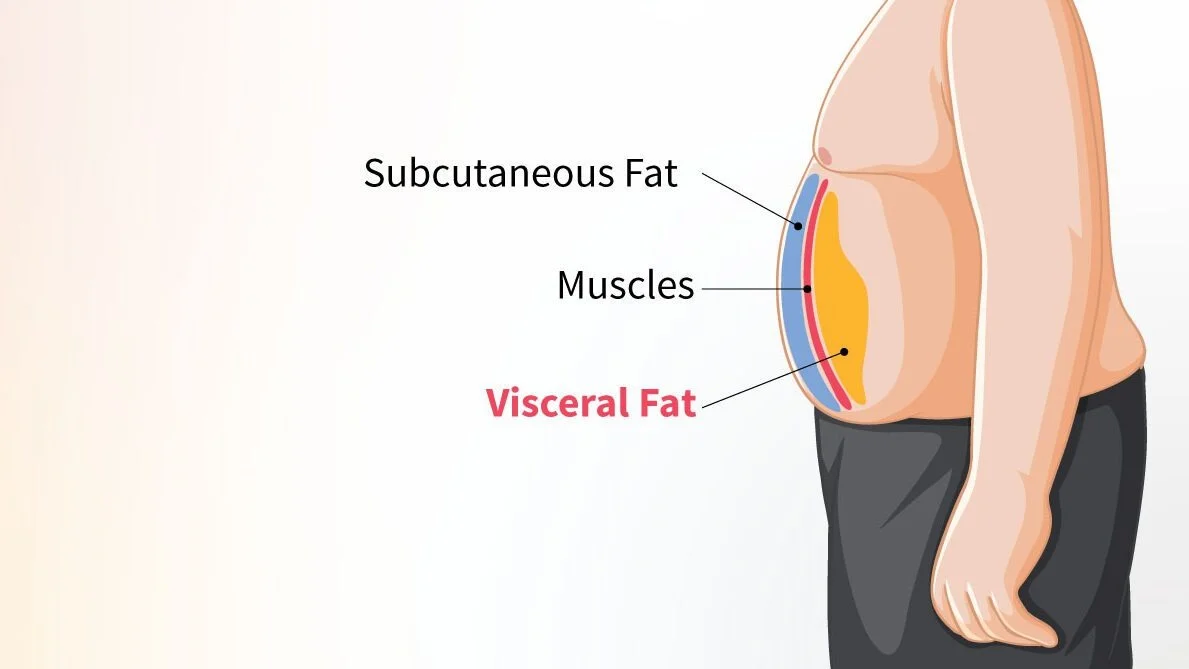
Your weighing scale cannot see it. Your BMI cannot find it. But visceral fat is silently working against your health right now. Unlike the fat you can see or pinch, visceral fat sits deep inside your abdominal cavity, wrapped around your liver, pancreas, and intestines. It is metabolically active. It releases harmful hormones. And for Indians especially, it accumulates at BMI levels that most doctors would call perfectly healthy.
This is not a condition that only affects people who look overweight. The ICMR-INDIAB 2025 study found that only 26.6% of Indian adults are truly metabolically healthy, meaning more than 7 in 10 Indians already carry at least one metabolic abnormality, often driven by excess visceral fat that no standard screening tool has ever detected. In this article, we break down the 7 serious health failures caused by high visceral fat and explain exactly what you can do to prevent each one.
- 73%Indians with at least one metabolic abnormality driven by visceral fat (ICMR-INDIAB 2025)
- 32%Indians with normal BMI but dangerously high visceral fat, the thin-fat phenotype
- 40% of Indian women have abdominal obesity driven by visceral fat (NFHS-5)
- $82BProjected annual cost of obesity to India’s economy by 2030 (from $29B in 2019)
What Is Visceral Fat, And Why Is It Different?
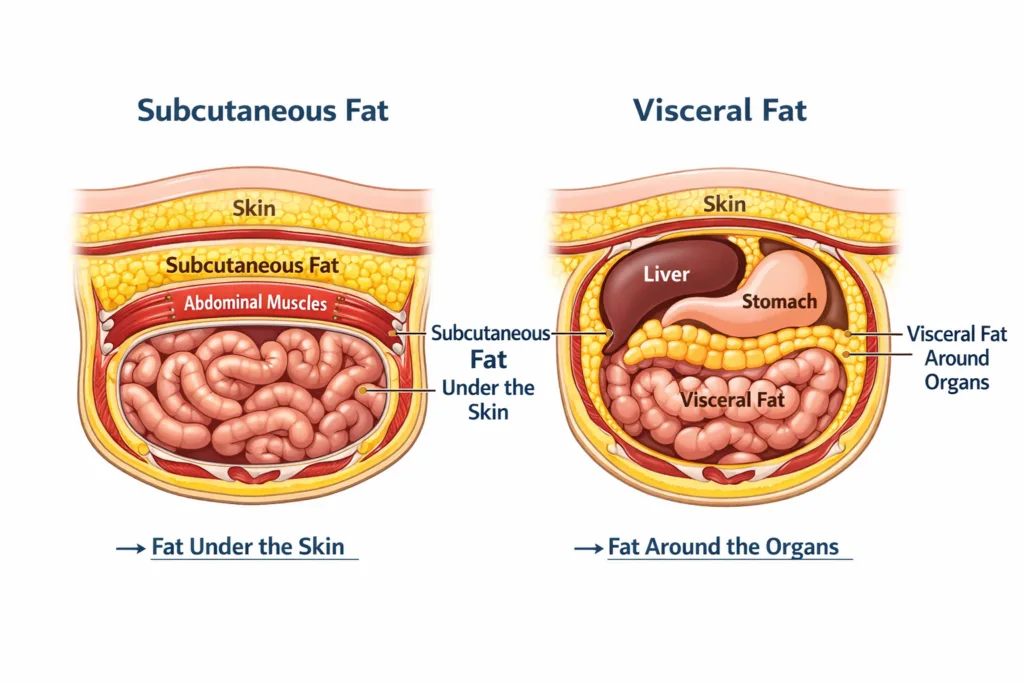
Not all fat is the same. Your body stores fat in two fundamentally different ways. Subcutaneous fat sits just under your skin the fat you can pinch on your belly, arms, or thighs. It is largely passive. Visceral fat is stored deep inside the abdominal cavity, packed tightly around your internal organs.
What makes visceral fat dangerous is that it behaves like an active endocrine organ. It secretes inflammatory cytokines, including interleukin-6 (IL-6) and tumour necrosis factor-alpha (TNF-α). It pumps free fatty acids directly into the portal vein, flooding the liver, and it disrupts insulin signalling at the cellular level. In short, visceral fat actively drives disease. It does not simply sit passively in your body the way subcutaneous fat does.
Why Indians Are At Higher Risk
South Asians genetically tend to store more fat around the abdomen and visceral organs even at lower body weights. A landmark PubMed study found that Indian men with a mean BMI of just 24.5 kg/m² had a mean body fat percentage of 33%, and 66% of them were already insulin-resistant. This is the core of the thin-fat Indian paradox: a normal BMI conceals a dangerously high-risk metabolic profile. Learn more about the thin-fat Indian phenotype.
1. Type 2 Diabetes: The Most Direct Link
The relationship between visceral fat and type 2 diabetes is the most well-established in metabolic medicine. Visceral fat releases free fatty acids directly into the portal circulation, triggering hepatic insulin resistance. At the same time, its inflammatory secretions impair glucose uptake in skeletal muscle, the tissue responsible for approximately 80% of insulin-stimulated glucose disposal in the body.
India is already the diabetes capital of the world, with 101 million people living with type 2 diabetes as of 2023. The ICMR-INDIAB study confirmed that Indians with the metabolically obese normal weight (MONO) phenotype, characterised by high visceral fat at normal BMI, had a significantly elevated risk of T2D, independent of total body weight. This means millions of Indians are developing diabetes while appearing completely healthy on paper.
Clinical Implication
Do not wait for BMI to rise before screening for diabetes risk. A patient with a Visceral Fat Level (VFL) of 10 or above on InBody should be assessed for insulin resistance regardless of BMI. InBody delivers this data in under 60 seconds, making it one of the most time-efficient metabolic screening tools available in outpatient practice today.
2. Cardiovascular Disease: The Silent Accelerator
Visceral fat accelerates cardiovascular disease through multiple simultaneous pathways. It raises LDL cholesterol and triglycerides, and lowers HDL cholesterol. It promotes systemic inflammation via C-reactive protein and IL-6. And it drives hypertension through activation of the renin-angiotensin system, all at the same time.
The ICMR-INDIAB 2025 analysis confirmed that the MONO phenotype metabolic obesity at normal weight, driven largely by visceral fat, was independently associated with elevated risk of coronary artery disease, even after controlling for total body weight. India already records over 579,000 adult deaths annually from NCDs attributable to overweight and obesity, with cardiovascular disease the leading cause.
What makes this especially alarming is that many of these patients have no visible obesity. Their ECG and BMI are normal. Their symptoms are absent. The risk is entirely hidden, and only body composition analysis can reveal it.

3. Fatty Liver Disease: India’s Fastest-Growing Silent Epidemic
Metabolically associated steatosis liver disease (MASLD), formerly known as NAFLD, is now the most common liver condition in India. Visceral fat is its primary driver. The free fatty acids released by visceral fat flow directly to the liver via the portal vein. There, they accumulate as hepatic triglycerides, triggering inflammation, fibrosis, and, over time, cirrhosis.
A 2025 study in India’s IT workforce found that 84% of IT employees had elevated liver fat accumulation. A separate nationwide analysis confirmed that visceral adiposity is the single strongest predictor of MASLD in Indian adults, stronger than total body weight, BMI, or waist circumference alone.
The liver damage from MASLD is silent for years. By the time elevated liver enzymes appear on a blood panel, significant steatosis has already occurred. Early detection through visceral fat screening before liver enzymes rise is the only way to intervene before structural damage begins.
Key Insight
Waist circumference alone underestimates visceral fat burden in Indians. A patient may have a waist measurement within normal limits yet carry dangerous levels of visceral fat concentrated around the liver. InBody measures Visceral Fat Level directly, providing the clinical precision that waist circumference and BMI simply cannot deliver.
4. Hypertension: The Visceral Fat–Blood Pressure Loop
Visceral fat activates the renin-angiotensin-aldosterone system (RAAS) the key hormonal pathway that controls blood pressure. Visceral adipocytes produce angiotensinogen, which drives vasoconstriction and sodium retention. At the same time, visceral fat-driven insulin resistance causes the kidneys to retain sodium further, pushing blood pressure higher still.
Lancet regional data on abdominal obesity in India found that 40% of Indian women and 12% of Indian men meet the criteria for abdominal obesity a direct proxy for high visceral fat. Among this group, hypertension prevalence is significantly elevated, even in those whose BMI would classify them as normal weight.
Consider this: a patient with BP of 138/88 mmHg and a BMI of 23.5 kg/m² may receive reassurance at a standard health check. Their Visceral Fat Level of 12, detectable only through body composition analysis, tells the real story behind their borderline hypertension.

5. Metabolic Syndrome: When Four Risks Arrive Together
Metabolic syndrome is defined as the co-occurrence of at least three of five risk factors: abdominal obesity, high triglycerides, low HDL cholesterol, elevated blood pressure, and elevated fasting glucose. Visceral fat is the central driver of all five. It does not cause them sequentially; it drives them simultaneously, through overlapping inflammatory and hormonal pathways.
The scale of this in India is striking. A 2025 IT workforce study found metabolic syndrome in 34.2% of employees all working age, most with normal or near-normal BMI, many completely unaware. The ICMR-INDIAB data confirms that Indians develop metabolic syndrome at lower BMI and younger ages than Western populations.
The Metabolic Syndrome Trap for Indians
Standard metabolic syndrome criteria use Western waist cut-offs (men: 102 cm, women: 88 cm). Indian-specific cut-offs are far lower for men: 90 cm, women: 80 cm, because Indians develop metabolic risk at smaller waist measurements. Using Western cut-offs in Indian clinical practice leads to systematic under-diagnosis in exactly the patients who need intervention most urgently.
6. Hormonal Disruption: The Impact Nobody Talks About
Visceral fat is not just stored fat. It is active and affects hormones in the body.
In women, too much visceral fat increases the conversion of male hormones into estrogen. This happens through enzymes called aromatase. As a result, it can lead to PCOS, irregular periods, and infertility. It can also raise cortisol levels. Because of this, the body stores even more visceral fat. Over time, this creates a cycle that is hard to break without targeting the fat itself.
In men, visceral fat lowers testosterone levels. It does this by increasing estrogen and affecting the testes. As testosterone drops, muscle mass decreases. At the same time, fat storage around the abdomen increases. This again creates a cycle where fat gain and hormone imbalance feed each other.
Therefore, many metabolic and hormonal problems often appear together in people with high visceral fat.
For doctors treating PCOS, infertility, or low testosterone, checking visceral fat is important. In other words, treating only the hormone problem is not enough. To get lasting results, the root cause visceral fat must also be addressed.

7. Cognitive Decline: The Brain–Belly Connection
The link between visceral fat and brain health is one of the most compelling and most underappreciated areas of metabolic research. Visceral fat drives systemic inflammation, and chronic low-grade inflammation is now recognised as a primary driver of neurodegeneration, cognitive decline, and dementia.
Multiple longitudinal studies confirm that high mid-life visceral fat is independently associated with smaller hippocampal volume, impaired memory consolidation, and increased Alzheimer’s risk even after controlling for cardiovascular risk factors. The mechanism involves visceral fat-derived IL-6 crossing the blood-brain barrier and triggering neuroinflammation.
For clinicians treating patients in their 30s and 40s, this is directly relevant. The visceral fat accumulating silently today in your patient with a normal BMI, a sedentary job, and a processed-food diet is the neurological risk factor of their 60s and 70s. Intervening now is not just about preventing diabetes. It is about protecting the brain.
The Good News
Of all fat depots in the body, visceral fat responds fastest to lifestyle intervention. Studies consistently show that a 5–7% reduction in body weight through diet and exercise produces a 30–40% reduction in visceral fat volume with measurable improvements in insulin sensitivity, blood pressure, and liver fat within 8–12 weeks. The key is measuring it so you can confirm it is actually changing.
Why BMI Cannot Detect Visceral Fat, and What Can
BMI uses only weight and height. It cannot distinguish fat from muscle. It cannot differentiate subcutaneous fat from visceral fat. And it has no ethnic correction for Indian patients who carry dangerous visceral fat levels at BMI values that Western guidelines call healthy.
The gold standard for visceral fat measurement is CT or MRI scanning, but these are expensive, time-consuming, and impractical for routine clinical use. InBody bioelectrical impedance analysis provides a clinically validated Visceral Fat Level score (1–20) in under 60 seconds, at 98.4% accuracy compared to DEXA, making it the only practical visceral fat screening tool for routine outpatient use in India.
Real Case: The Patient With ‘Nothing Wrong’ Until InBody Scanned
A 42-year-old software engineer in Hyderabad came in for a corporate health check. His BMI was 24.1, fasting glucose was 98 mg/dL and blood pressure was 132/84 mmHg. On every standard metric, he was borderline at worst, and his previous doctor had told him there was nothing to worry about.
His InBody scan told a completely different story. It revealed a Visceral Fat Level of 13 (high risk), a Body Fat Percentage of 31.2% (obese by composition using IAP reference values), and Skeletal Muscle Mass 1.8 kg below the population norm for his height and age. He was a textbook presentation of metabolic obesity at normal weight, and his cumulative risk for type 2 diabetes and cardiovascular disease placed him firmly in the high-risk category.
After a 12-week programme of resistance training three times per week, reduced refined carbohydrate intake, and improved sleep, his follow-up InBody scan showed the following changes:
- ↓3 units Visceral Fat Level (13 → 10)
- +1.4 kg Skeletal Muscle Mass gained
- ↓3.8%Body Fat Percentage reduced
Normal fasting glucose and BP at 12 weeks
His BMI had moved by just 0.3 units over the same period. Without the InBody data, there would have been no evidence that anything had changed and no clinical motivation to continue. Body composition data changed both the diagnosis and the outcome.
How to Reduce Visceral Fat: 6 Evidence-Based Steps
Visceral fat responds to lifestyle intervention faster than any other fat depot in the body. These are the six interventions with the strongest clinical evidence for visceral fat reduction in Indian adults.
- Aerobic exercise 150 to 300 minutes per week. Moderate-intensity aerobic activity (brisk walking, cycling, swimming) produces consistent visceral fat reduction independent of dietary change. Even 150 minutes per week produces measurable VFL reduction within 8 weeks.
- Resistance training 2 to 3 sessions per week. Building skeletal muscle mass increases basal metabolic rate and glucose disposal capacity, creating a metabolic environment that reduces visceral fat actively even at rest. This is especially important for Indian patients with the thin-fat phenotype.
- Reduce refined carbohydrates and added sugars. Refined carbohydrates drive hepatic de novo lipogenesis, the liver’s conversion of excess glucose into fat, which deposits preferentially as visceral and hepatic fat. Replacing white rice, maida, and sweetened beverages with whole grains, pulses, and water produces measurable visceral fat reduction within 12 weeks.
- Adequate sleep is 7 to 9 hours per night. Sleep deprivation elevates cortisol, which directly stimulates visceral fat deposition. A consistent sleep deficit of even 1–2 hours per night produces significant accumulation over months.
- Stress management. Chronic psychological stress is an independent driver of visceral fat through cortisol-mediated adipogenesis. Yoga, mindfulness-based stress reduction (MBSR), and structured relaxation techniques have all demonstrated visceral fat reduction in controlled trials.
- Track progress with body composition analysis. Without measurement, patients cannot see visceral fat changing even as their metabolic health improves. Regular InBody scanning every 8–12 weeks provides the data that motivates continued adherence and guides clinical adjustments.

Frequently Asked Questions
Visceral fat is fat stored deep inside the abdominal cavity, surrounding your liver, pancreas, and intestines. Unlike subcutaneous fat under the skin, visceral fat is metabolically active; it releases inflammatory cytokines, disrupts insulin signalling, and directly drives type 2 diabetes, cardiovascular disease, and fatty liver disease. You cannot see it, feel it, or measure it on a weighing scale.
On InBody devices, a Visceral Fat Level (VFL) of 1–9 is considered normal, 10–14 is high risk, and 15–20 is very high risk. For Indian patients, clinical intervention should be considered from VFL 10 onwards. Indians develop metabolic disease at lower visceral fat thresholds than Western populations due to the thin-fat phenotype.
Yes, and this is extremely common in India. Approximately 32% of Indians have normal BMI but high visceral fat and significant metabolic risk. A weighing scale or BMI calculation cannot detect visceral fat. Only body composition analysis, such as InBody BIA, can measure it directly. A Gujarat-based study found that 45% of normal-BMI participants had high body fat and visceral fat, with 50% showing elevated fasting glucose.
Visceral fat responds faster to lifestyle intervention than subcutaneous fat. Evidence-based strategies include 150–300 minutes of moderate aerobic exercise per week, progressive resistance training 2–3 times per week, a diet low in refined carbohydrates and added sugars, 7–9 hours of sleep, and stress management. A 5–7% reduction in body weight produces a 30–40% reduction in visceral fat volume. Regular InBody scanning every 8–12 weeks tracks this reduction objectively.
The gold standard is CT or MRI scanning. However, InBody bioelectrical impedance analysis (BIA) provides a clinically validated Visceral Fat Level score (1–20) in under 60 seconds, at 98.4% accuracy compared to DEXA, making it the most practical tool for routine clinical visceral fat screening in India. It is non-invasive, radiation-free, and the results are available immediately.
Key Takeaways
- Visceral fat is invisible to BMI, the weighing scale, and standard blood tests, yet it is the single most dangerous fat depot in the body.
- It simultaneously drives 7 serious health conditions: type 2 diabetes, cardiovascular disease, fatty liver disease, hypertension, metabolic syndrome, hormonal disruption, and cognitive decline.
- 32% of Indians with normal BMI carry dangerously high visceral fat, the thin-fat Indian phenotype that standard screening completely misses.
- InBody delivers a direct Visceral Fat Level score (1–20) in under 60 seconds at 98.4% accuracy the only practical visceral fat screening tool for routine clinical use in India today.
- A 5–7% reduction in body weight produces a 30–40% reduction in visceral fat, but you can only confirm it is actually decreasing through regular body composition analysis.
- Every patient with borderline glucose, hypertension, dyslipidaemia, or PCOS deserves a visceral fat assessment regardless of what their BMI says.
An InBody scan takes under 60 seconds and gives you a direct Visceral Fat Level score that your weighing scale will never show you. Available at hospitals, fitness centres, and corporate wellness facilities across India.
Find an InBody Scanner Near You
References & Further Reading
- ICMR-INDIAB Study 2025. High prevalence of metabolic obesity in India. Indian Journal of Medical Research. 2025.
- Lancet Regional Health — Southeast Asia. Abdominal obesity in India: NFHS-5 analysis. 2023.
- PMC. Obesity and Abdominal Obesity in the Indian Population — NFHS-5 nationally representative study. 2023.
- Clinical Obesity / PMC. Burden of Obesity in India: Need for Policy Changes. 2026.
- Banerji MA et al. Body composition, visceral fat, leptin, and insulin resistance in Asian Indian men. J Clin Endocrinol Metab. 1999.
- Scientific Reports. Prevalence of MAFLD among IT employees in India. Nature. 2025.
- ADA. Body Composition in South Asian Indian Population — The Gujarat Phenotype. Diabetes. 2025.
- Misra A et al. Consensus statement for the diagnosis of obesity for Asian Indians. JAPI. 2009.
Related:
Body Fat Percentage — Normal Ranges for Indians |
Compare InBody Models |
Find an InBody Test Centre Near You

Most trending articles

Post-Pregnancy Weight Loss in India — Why the Scale Lies
Post-pregnancy weight loss is not about the scale. For Indian mothers, the real story is muscle, fat and water — and rebuilding them in the right order.

Type 2 Diabetes & Body Composition (India 2026 Guide)
India has 101 million diabetics, and many are "thin." Body composition explains what BMI and HbA1c miss — and what to actually track for control and remission.
PCOD Management in India — What Body Composition Tells You
PCOD affects 1 in 5 Indian women. "Lose weight" is the wrong first instruction. Here is what body composition adds — and a 6-month plan that actually works.