Fitness 14 min read
Is Pilates the Secret to a Stronger, Leaner You?
You go to the gym three times a week, track your workouts. You feel like you are doing everything right. Yet your lower back aches, your posture is collapsing,…
Reading about body composition? Find an InBody test centre near you →
You go to the gym three times a week, track your workouts. You feel like you are doing everything right. Yet your lower back aches, your posture is collapsing, your energy is flat, and your last health check showed nothing obviously wrong. The problem may not be that you are not exercising enough. The problem may be that your gym routine is actively undermining the very muscles it is supposed to build.
This is not a niche edge case. Data from the InBody–Ipsos 2020 study conducted across 1,243 Indian adults in eight cities found that 71% of Indian adults aged 30–55 have poor skeletal muscle mass, including large numbers who exercise regularly. The reason is structural: most common gym routines contain hidden design flaws that reduce core skeletal muscle mass over time, even in consistent exercisers.
This article explains exactly what those flaws are, what the clinical evidence says about them, and critically, how body composition analysis detects the damage before symptoms progress into diagnosis.
| 71% Indians aged 30–55 have poor muscle health, InBody–Ipsos study, 2020 | 80% Of insulin-stimulated glucose uptake is handled by skeletal muscle, low core = diabetes risk | 3–5% Muscle loss per decade in sedentary adults doubles after age 60 | 73% Indian households are consuming below the minimum daily protein requirement, IMRB survey, 2020 |
NOTE FOR MEDICAL PRACTITIONERS
This article draws on the InBody–Ipsos 2020 study (n=1,243, 8 Indian cities, age 30–55), peer-reviewed sarcopenia and exercise physiology literature, and AWGS 2019 consensus guidelines. All InBody metrics referenced SMM, SMI, ECW/TBW, and Segmental Lean are produced by Direct Segmental Multi-frequency BIA at 98.4% correlation accuracy versus DEXA. Clinical references are listed at the end of this article.
Why the Gym Can Hurt Your Core And Why Most People Never Know
The common assumption is that any exercise is better than no exercise for muscle health. In terms of cardiovascular fitness, that is broadly true. For skeletal muscle mass, however, it is not. Muscle responds specifically to the type, frequency, and volume of mechanical load it receives. The wrong programme design does not just fail to build muscle, it can accelerate the very muscle loss it is meant to prevent.
The deeper problem is that standard assessments cannot detect this. Weight stays the same. BMI stays the same. Blood tests show nothing abnormal. The only way to see that core skeletal muscle is declining is to measure body composition directly, which is precisely what most gym-goers and most health check-ups never do.

7 Urgent Reasons Your Gym Routine Is Sabotaging Your Core Muscle
1. You Are Doing Too Much Cardio and Not Enough Resistance Training
Long-duration, steady-state cardio treadmill runs, elliptical sessions, and cycling classes are the default activities in most Indian gym routines. It is excellent for cardiovascular health. However, it is not a stimulus for skeletal muscle protein synthesis. In fact, when performed in excess without counterbalancing resistance work, sustained cardio elevates cortisol, a catabolic hormone that breaks down muscle tissue for energy.
Research published in the Journal of Strength and Conditioning Research confirms that concurrent training (cardio plus resistance in the same session) reduces the hypertrophic signal of resistance work, a phenomenon called the interference effect. For Indian adults already protein-deficient and carrying the thin-fat phenotype, excessive cardio without resistance training is a direct pathway to progressive core muscle loss, even while body weight remains unchanged.
THE FIX
Limit steady-state cardio to 20–30 minutes per session. Prioritise progressive resistance training for at least two of every three gym sessions. Monitor the result on your Segmental Lean (Trunk) score on an InBody scan every 8–12 weeks.
2. You Are Using Machines Instead of Compound Movements
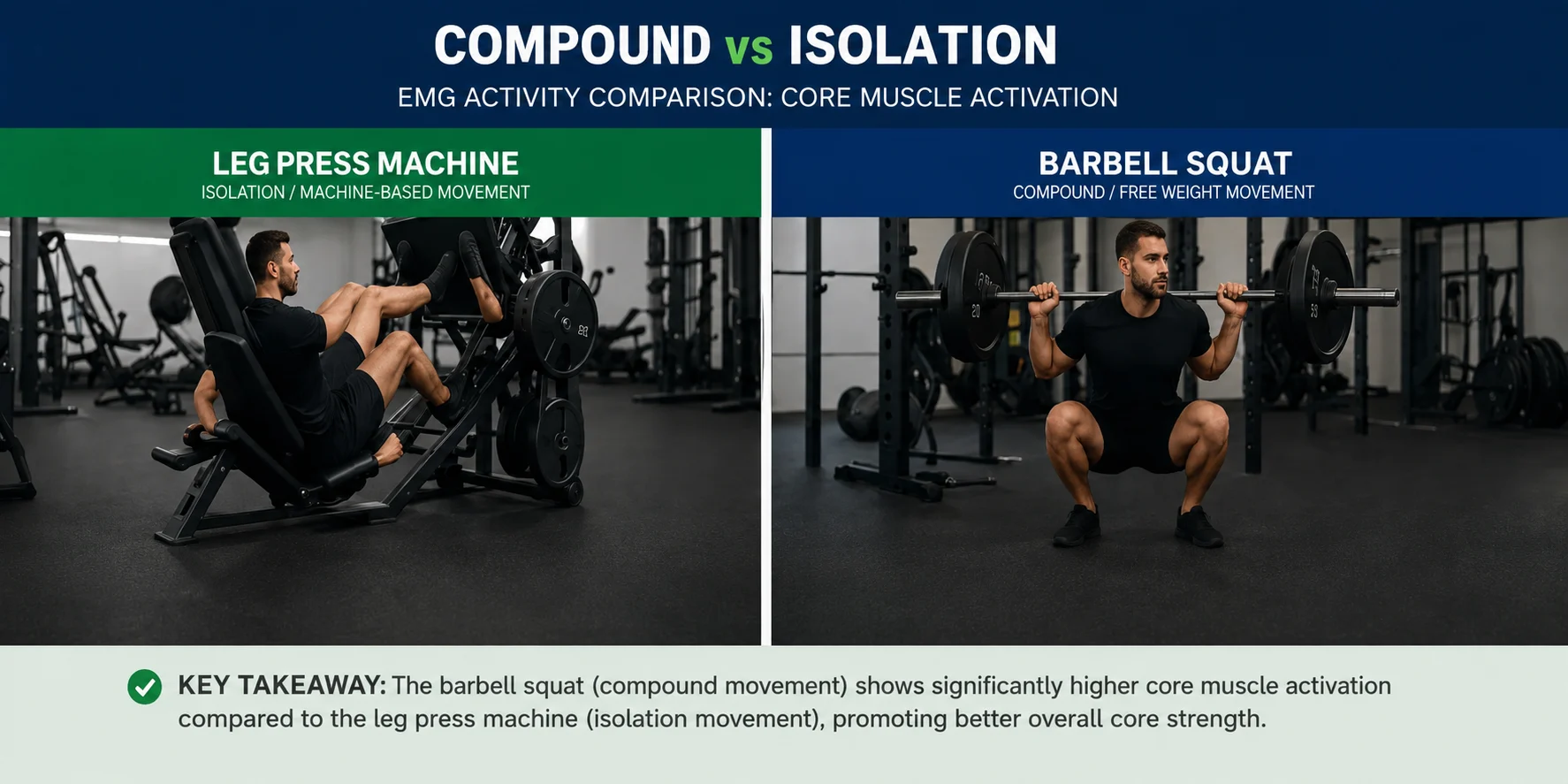
Isolation machines leg extension, pec deck, and lat pulldown are popular in Indian gyms because they feel safe and comfortable. The problem is that they train individual muscle groups in fixed planes, providing minimal recruitment of the deep core stabilisers, the transverse abdominis, multifidus, quadratus lumborum, and pelvic floor.
Compound free-weight movements, such as squats, deadlifts, Romanian deadlifts, overhead press, and barbell rows, require the entire core to co-activate as a stabilising system. Studies on core electromyography consistently show that free-weight compound lifts activate significantly more trunk muscle fibres than isolated machine equivalents. A gym routine built entirely on machines will produce localised hypertrophy while leaving the functional core, the muscles responsible for spinal stability, posture, and glucose disposal, undertrained and progressively weakened.
THE FIX
Include at least two compound lower-body movements (squats, deadlifts) and one compound pressing or pulling movement in every resistance session. These are the highest-value exercises for core skeletal muscle mass in the InBody Segmental Trunk and Leg readings.
3. Your Post-Workout Protein Intake Is Critically Insufficient
Exercise creates a catabolic stimulus it breaks muscle fibres down. Muscle growth occurs only during the recovery window that follows, and only when sufficient dietary protein is available to drive muscle protein synthesis. Without that protein, exercise produces a net catabolic result: you have stressed the muscle without giving it the raw material to rebuild.
The post-exercise anabolic window, the period of elevated muscle protein synthesis sensitivity following resistance training, lasts approximately 24–48 hours. During this window, the recommended protein intake is 1.6–2.0 g/kg of body weight per day. Yet the average Indian adult consumes approximately 0.6 g/kg/day, barely one-third of what is needed for adequate recovery. For a 70 kg Indian adult who trains three times per week, this means their body is attempting to rebuild stressed muscle tissue on a protein deficit at every single session.
THE FIX
Target a minimum of 1.4–1.6 g of protein per kg of body weight per day on training days. On a 70 kg frame, this means 98–112 g of protein daily. Distribute across three meals: eggs, paneer, curd, chicken, fish, soya chunks, and dal combined with rice are the highest-quality Indian sources.
4. You Are Neglecting the Posterior Chain the Foundation of Core Strength
Most gym programmes in India are anterior-dominant: they train the chest, biceps, and quadriceps far more than the glutes, hamstrings, erector spinae, and rhomboids. This creates a muscular imbalance that is clinically significant. The posterior chain the muscles running from your calves up through your hamstrings, glutes, and lower and upper back is the primary load-bearing structure that supports the spine and pelvis.
When the posterior chain is weak relative to the anterior muscles, the pelvis tilts forward (anterior pelvic tilt), the lumbar spine hyperlordosis, and the true deep core stabilisers become inhibited. The result is chronic lower back pain, poor posture, reduced functional strength, and, critically, progressive loss of the trunk skeletal muscle mass that InBody measures as Segmental Lean (Trunk). This pattern is extremely common in Indian gym-goers and is rarely identified by standard health assessments.
THE FIX
Ensure your weekly programme includes dedicated posterior chain work: Romanian deadlifts, hip thrusts, barbell rows, face pulls, and back extensions. Target a posterior-to-anterior training ratio of at least 1:1 in terms of volume.
5. You Are Training Without Progressive Overload So Adaptation Has Stalled
Skeletal muscle adapts to the stress placed upon it. Once it has adapted to a given load, continued exposure to that same load produces no further hypertrophic stimulus. This is the principle of progressive overload: muscle only grows when the demand on it increases systematically over time.
Studies in exercise physiology show that muscle adaptation to a constant resistance load plateaus within 6–8 weeks. After that point, maintaining the same weight, sets, and repetitions produces no further increase in skeletal muscle mass and without dietary protein to even sustain current mass, modest muscle loss resumes. The vast majority of Indian gym-goers who have been doing the same routine for months or years are in this stalled state, experiencing the metabolic consequences of low core muscle mass despite attending the gym regularly.
THE FIX
Use a structured progressive overload method: add 2.5–5 kg to compound lifts every two to four weeks, or increase repetitions from 8 to 12 before adding weight. Track your progress and measure the outcome every 12 weeks with an InBody scan. The Skeletal Muscle Mass and InBody Score numbers will confirm whether adaptation is occurring.
6. You Are Chronically Under-Recovering, and Cortisol Is Destroying Your Core
Recovery is when muscle is built. Training is merely the stimulus. When sleep is insufficient, stress is chronically elevated, or rest days are inadequate, cortisol remains elevated and elevated cortisol is directly catabolic to skeletal muscle tissue. It accelerates muscle protein breakdown, suppresses insulin-like growth factor-1 (IGF-1), and redirects amino acids away from muscle protein synthesis toward gluconeogenesis.
India’s urban professional population, the same demographic identified in the InBody–Ipsos study, is also among the most sleep-deprived and chronically stressed in the world. Sleeping fewer than seven hours per night has been shown to reduce muscle protein synthesis by up to 18% compared to adequate sleep, independent of training and diet. An Indian IT professional who trains hard but sleeps six hours and works under chronic deadline pressure may be experiencing net muscle loss despite their gym attendance.
Furthermore, the ECW/TBW ratio on an InBody scan, the extracellular-to-total body water ratio rises with chronic inflammation and stress-related fluid shifts. This marker detects the physiological burden of chronic under-recovery before it manifests as clinical symptoms.
THE FIX
Prioritise 7–9 hours of sleep per night. Include at least two full rest days per week. Monitor your ECW/TBW ratio at every InBody scan as an objective marker of recovery quality. A rising ratio signals the need to reduce training volume or address sleep and stress.
7. You Are Measuring the Wrong Things and Missing the Evidence of Muscle Loss
The most insidious reason gym routines sabotage core muscle is that the tools most people use to assess their progress, weighing scales and BMI, are structurally incapable of detecting the problem. Body weight does not distinguish between muscle, fat, water, and bone. BMI rises when you gain muscle and falls when you lose it, providing actively misleading feedback.
This measurement gap is especially damaging for Indian adults because of the thin-fat Indian phenotype, the well-documented tendency of South Asians to carry lower muscle mass and higher visceral fat at the same BMI compared to Western populations, first described by Professor C.S. Yajnik at KEM Hospital Pune. An Indian gym-goer losing core muscle while gaining visceral fat can show an unchanged body weight and an unchanged BMI for months right up to the point where metabolic consequences become clinically apparent.
The only tool that detects this pattern early is direct body composition analysis. InBody’s Direct Segmental Multi-frequency BIA measures skeletal muscle mass in kilograms, broken down by trunk and limb segments, and compares it against age- and sex-adjusted Indian population norms in under 60 seconds, with no radiation and no blood draw.
THE FIX
Replace weight tracking with InBody Score tracking. Measure every 8–12 weeks during active training. Track Skeletal Muscle Mass (SMM), Segmental Lean (Trunk and Legs), Skeletal Muscle Index (SMI), and ECW/TBW ratio at every scan. These numbers tell you whether your gym routine is actually building or depleting the core muscle that your long-term health depends on.
What InBody Detects That Your Gym Progress Photos Cannot
Body composition analysis using InBody’s Direct Segmental Multi-frequency BIA (DSM-BIA) produces five metrics that are directly relevant to identifying gym-related core muscle sabotage. Each metric provides information that no fitness tracker, smartwatch, weighing scale, or blood panel can supply.
| InBody Metric | What It Reveals | Clinical Significance for Gym-Goers |
|---|---|---|
| Skeletal Muscle Mass (SMM) | Total lean muscle in kg vs. population norm for age, sex, and height | Primary indicator of whether training is producing net muscle gain or loss |
| Segmental Lean Analysis | Muscle breakdown by right arm, left arm, trunk, right leg, left leg | Identifies imbalances; the trunk segment directly measures core muscle status |
| Skeletal Muscle Index (SMI) | Appendicular muscle ÷ height² vs. AWGS sarcopenia threshold (7.0 m/kg² men; 5.4 f/kg² women) | Clinical sarcopenia screen: flags early sarcopenia in gym-goers who appear fit |
| ECW/TBW Ratio | Extracellular-to-total body water ratio; rises with inflammation and chronic stress. | Objective marker of under-recovery; rises before symptoms appear |
| InBody Score | Composite 0–100 muscle-fat balance index | Single trackable progress number; above 80 = healthy composition; below 70 = clinically relevant imbalance |
CLINICAL PROTOCOL: MONITORING GYM-GOING PATIENTS FOR CORE MUSCLE LOSS
For Indian adult patients aged 30–55 who exercise regularly but present with fatigue, back pain, poor recovery, or metabolic concerns, the following InBody monitoring schedule is recommended:
Baseline scan → before or at start of any structured training programme
8-week scan → assess early adaptation; flag stalled or negative SMM trend
16-week scan → confirm sustained muscle gain trajectory
Ongoing → every 12–16 weeks for active exercisers; every 6 months for maintenance
Real-World Case: The Regular Gym-Goer With Declining Core Muscle
A 38-year-old female marketing professional in Mumbai had been attending a gym five times per week for over two years. Her routine consisted predominantly of treadmill running (45 minutes), group fitness classes, and occasional machine-based resistance work. She reported persistent lower back pain, fatigue by mid-afternoon, and difficulty maintaining posture during long seated meetings. Her BMI was 22.4, well within the normal range, and her last standard health check had returned entirely normal results.
An InBody 770 scan at a corporate wellness clinic revealed a clinical picture that her BMI and blood results had completely obscured. Specifically, it showed Skeletal Muscle Mass 3.6 kg below the population norm for her age and height, a Segmental Lean Trunk score at the lower boundary of the normal range, a Visceral Fat Level of 9 (borderline high), and an ECW/TBW ratio of 0.388, indicating subclinical inflammation. She met the criteria for pre-sarcopenic muscle deficit at 38 years old, despite five gym sessions per week.
A 16-week programme correction was initiated: three weekly resistance sessions replacing two cardio sessions, dietary protein increased to 1.5 g/kg/day, and Vitamin D and magnesium supplementation to address confirmed deficiencies. The 16-week follow-up InBody scan results were clinically meaningful across every tracked marker:
| +2.9 kgSkeletal Muscle Mass gained | ↓2 units Visceral Fat Level (9 → 7) | 0.381ECW/TBW ratio reduced inflammation | 79 → 86InBody Score improvement |
Her lower back pain resolved within eight weeks. Afternoon fatigue lifted by week twelve, and posture improved measurably. This case is representative of a pattern seen consistently across Indian corporate wellness and clinical settings: regular gym attendance does not guarantee adequate core muscle mass, and the tools most people use to track fitness are incapable of revealing that.
Who Should Get an InBody Scan Even If They Already Exercise
Given that 71% of Indian adults have poor muscle health regardless of exercise habits, the practical answer is that any Indian adult over 30 who exercises without objective body composition data is training without evidence. However, the following groups have the highest clinical priority for immediate screening.
| Patient Group | Why They Are at Risk |
|---|---|
| Regular gym-goers with persistent fatigue or back pain | These symptoms frequently signal core muscle deficit masked by normal body weight and BMI |
| Adults doing primarily cardio without resistance training | High cortisol + insufficient mechanical load = net muscle loss over time |
| Patients with prediabetes or metabolic syndrome | The core muscle is the primary glucose disposal organ; low SMM directly drives insulin resistance. |
| Post-weight-loss patients (diet or surgery) | Rapid weight loss commonly destroys muscle alongside fat; body composition confirms whether lean mass is preserved. |
| Women over 40 | Declining oestrogen significantly accelerates muscle loss; exercise alone cannot compensate without adequate protein and resistance loading. |
| Desk-based professionals aged 30–55 | India’s IT and finance professionals combine sedentary occupations with protein-deficient diets, the highest-risk profile in the InBody–Ipsos study. |
Key Takeaways for Clinicians and Patients
- Regular gym attendance does not guarantee adequate core muscle mass. 71% of Indian adults aged 30–55 have poor skeletal muscle health, including many who exercise consistently InBody–Ipsos 2020 study.
- The seven hidden gym mistakes, excess cardio, machine-only training, post-workout protein deficit, posterior chain neglect, absence of progressive overload, chronic under-recovery, and wrong measurement tools, collectively drive core muscle loss in otherwise active individuals.
- BMI and body weight cannot detect core muscle decline. An InBody body composition scan measures Skeletal Muscle Mass directly, against age- and sex-adjusted Indian norms, in under 60 seconds.
- The thin-fat Indian phenotype means that normal BMI actively conceals core muscle deficit in South Asian adults. Body composition analysis is not optional for this population; it is clinically necessary.
- Core muscle loss is highly reversible with corrected programme design, progressive resistance training three times per week plus 1.4–1.6 g/kg/day protein producing measurable InBody gains within 8–12 weeks.
- Clinical monitoring using InBody SMM, Segmental Lean (Trunk), SMI, ECW/TBW ratio, and InBody Score provides the only objective evidence of whether a training programme is achieving its intended metabolic outcome.
Find Out Whether Your Gym Routine Is Building or Destroying Your Core
An InBody scan takes under 60 seconds and gives you the precise muscle health data that no scale, fitness tracker, or blood test can provide.

Find an InBody Scanner Near You
References & Clinical Sources
- InBody and Ipsos. “71% Indians suffer from poor muscle health.” Joint study across 8 Indian cities, n=1,243. November 2020.
- Asian Working Group for Sarcopenia. “2019 Consensus Update on Sarcopenia Diagnosis and Intervention.” Journal of the American Medical Directors Association. 2020.
- DeFronzo RA et al. “Skeletal muscle insulin resistance is the primary defect in type 2 diabetes.” Diabetes Care. 2009.
- Yajnik CS, Yudkin JS. “The Y-Y paradox.” The Lancet. 2004;363(9403):163.
- Kim TN, Choi KM. “Sarcopenia: Definition, epidemiology, and pathophysiology.” Journal of Bone Metabolism. 2013.
- Wilson JM, et al. “Concurrent training: a meta-analysis examining interference of aerobic and resistance exercises.” Journal of Strength and Conditioning Research. 2012;26(8):2293–2307.
- Schoenfeld BJ. “The mechanisms of muscle hypertrophy and their application to resistance training.” Journal of Strength and Conditioning Research. 2010;24(10):2857–2872.
- Dattilo M, et al. “Sleep and muscle recovery: endocrinological and molecular basis for a new and promising hypothesis.” Medical Hypotheses. 2011;77(2):220–222.
- InBody Co. “Validation of InBody BIA against DEXA in diverse clinical populations.” InBody White Paper Series. Seoul: InBody Co., 2022.
- Misra A, et al. “Consensus statement for diagnosis of obesity and metabolic syndrome for Asian Indians.” JAPI. 2009.

Most trending articles

Fitness After 60: The Body Composition Guide for India’s Growing Senior Population
India will have 300 million seniors by 2050. The biggest threat isn't disease — it's muscle loss. Body composition testing after 60 reveals the exact protocol to stay strong, independent, and healthy well into old age.

Low Testosterone in Indian Men: How It’s Destroying Muscle Mass (And What Body Composition Shows)
Indian men's testosterone levels are declining. Low T causes muscle loss, visceral fat gain, and metabolic slowdown. How body composition testing is the first sign of testosterone decline — years before blood tests flag it.

Keto Diet in India: What Happens to Your Body Composition (The Real Data, Not the Hype)
Keto is India's most-googled diet. But what does body composition testing show after 8 weeks on keto? Rapid fat loss or dangerous muscle loss? The India-specific guide to keto with body composition tracking.