Body Composition 18 min read
India’s Muscle Health Crisis: Causes, Risk & How to Reverse It
Seven out of every ten Indians have poor muscle health. That is not a projection or an estimate. It is the finding of a real study, conducted by…
Reading about body composition? Find an InBody test centre near you →
Seven out of every ten Indians have poor muscle health. That is not a projection or an estimate. It is the finding of a real study, conducted by InBody and Ipsos across 1,243 adults in eight Indian cities. Yet most Indians have never heard about it, most doctors do not routinely screen for it, and most health programmes in India are still focused almost entirely on weight and fat. Consequently, the muscle mass crisis is silently driving India’s epidemics of fatigue, diabetes, metabolic syndrome, and frailty and going largely unaddressed.
This article explains exactly why muscle loss is so prevalent in India, what it means for your health, how body composition analysis detects it before symptoms appear, and five practical, evidence-based steps that genuinely reverse it. Furthermore, it is written for both medical practitioners and informed patients because solving this problem requires both clinical tools and individual action.
| 71% Indians with poor muscle health InBody-Ipsos study, 2020, across 8 cities | 82% Males in Lucknow with poor muscle mass highest rate among all cities studied | 17.5% Indians aged under 65 already meeting clinical criteria for sarcopenia | 80% Of insulin-stimulated glucose uptake handled by skeletal muscle low muscle = diabetes risk |
NOTE FOR MEDICAL PRACTITIONERS
This article draws on the InBody-Ipsos 2020 study (n=1,243 adults, 8 Indian cities, age 30–55), published peer-reviewed sarcopenia literature, and AWGS 2019 consensus guidelines. All clinical claims are referenced at the end of this article. The InBody body composition metrics referenced SMM, SMI, ECW/TBW, and PBF are produced by Direct Segmental Multi-frequency BIA at 98.4% accuracy compared to DEXA.
The InBody-Ipsos Study: What the Data Actually Shows
The InBody-Ipsos study is the most comprehensive published dataset on Indian muscle health to date. Conducted across Delhi-NCR, Mumbai, Kolkata, Chennai, Ahmedabad, Lucknow, Patna, and Hyderabad, it measured body composition using clinical-grade InBody devices in 1,243 adults aged 30–55. The findings were, by any measure, alarming.
Overall, 71% of Indian adults had poor muscle mass, defined as skeletal muscle mass below the population norm for their age, sex, and height. Moreover, body protein levels followed the same pattern: the majority of respondents had protein levels below the clinical threshold for adequate muscle maintenance. Notably, the city-level data revealed significant geographic variation, with Lucknow recording the highest rates, 82% of males and 80% of females and Delhi-NCR recording the lowest at 64%.
Furthermore, this was not a study of elderly patients or hospital populations. These were working-age adults between 30 and 55, the most economically active demographic in India. In other words, the muscle mass crisis is not a fringe geriatric concern. It is a mainstream, working-age, nationwide public health failure.
Why Muscle Mass Is Not Just a Fitness Metric: It Is a Medical One
Muscle is still widely misunderstood by the public and, increasingly, by non-specialist clinicians as a performance tissue relevant only to athletes. In reality, skeletal muscle is a metabolically active organ system that regulates glucose disposal, immune function, bone health, hormonal balance, and long-term survival. Consequently, low muscle mass is not simply a fitness problem. It is a clinical risk factor for some of India’s most prevalent and costly diseases.
Muscle Mass and Type 2 Diabetes Risk
Skeletal muscle is responsible for approximately 80% of insulin-stimulated glucose uptake in the body. Therefore, when muscle mass is low, the body’s primary mechanism for clearing blood glucose is structurally compromised regardless of body fat levels or BMI. As a result, low skeletal muscle mass is now recognised as an independent risk factor for Type 2 diabetes, separate from obesity.
Moreover, the relationship is bidirectional. Patients with Type 2 diabetes lose thigh muscle at twice the rate of non-diabetic individuals. Furthermore, lower leg muscle mass is now considered an early indicator of insulin resistance detectable through body composition analysis before blood glucose abnormalities appear on standard tests. In other words, body composition screening catches diabetes risk earlier than HbA1c or fasting glucose alone.
Sarcopenia: When Muscle Loss Becomes a Clinical Diagnosis
Sarcopenia is the clinical diagnosis for pathologically low skeletal muscle mass and strength. According to the Asian Working Group for Sarcopenia (AWGS) 2019 guidelines, the threshold is a Skeletal Muscle Index (SMI) below 7.0 kg/m² in men and 5.4 kg/m² in women. Critically, AWGS uses Asian-specific reference values because Western sarcopenia thresholds systematically underdiagnose the condition in Indian and South Asian patients.
In India, sarcopenia currently affects an estimated 17.5% of adults under 65, a figure that is climbing rapidly due to sedentary urban lifestyles, protein-deficient diets, and an ageing population. Additionally, sarcopenia is strongly associated with falls, fractures, cognitive decline, poor surgical outcomes, and mortality. Consequently, early detection and reversal are among the highest-value clinical interventions available in preventive medicine in India today.
Muscle, Basal Metabolic Rate, and Body Fat Gain

Skeletal muscle is a metabolically expensive tissue it burns calories at rest. Therefore, as muscle mass declines, Basal Metabolic Rate (BMR) falls proportionally. The result is a gradual, self-reinforcing cycle: less muscle → lower BMR → easier fat gain → more weight on an already undertreated frame → further inactivity → further muscle loss.
This cycle is particularly insidious in Indian patients because of the thin-fat Indian phenotype, individuals who appear slim but carry high visceral fat and low muscle simultaneously. Standard BMI and weight measurements completely miss this pattern. In contrast, InBody body composition analysis detects it directly, in under 60 seconds.
| Consequence of Low Muscle Mass | Clinical Mechanism | Detectable via InBody? |
|---|---|---|
| Type 2 Diabetes | 80% of glucose uptake occurs in muscle, low SMM = insulin resistance | Skeletal Muscle Mass (SMM) |
| Sarcopenia and Frailty | SMI below AWGS threshold → loss of strength and functional independence | Skeletal Muscle Index (SMI) |
| Visceral Fat Accumulation | Lower BMR from muscle loss → fat replaces muscle compartment | Visceral Fat Level (VFL) |
| Chronic Fatigue | Insufficient myokine output and reduced cellular energy capacity | ECW/TBW Ratio |
| Falls and Fractures | Reduced leg muscle mass → impaired balance and load-bearing capacity | Segmental Lean Analysis |
| Poor Immune Function | Muscle is primary glutamine reservoir for lymphocytes and macrophages | SMM + ECW/TBW Ratio |
Why India Specifically Has a Muscle Mass Problem
Poor muscle health is a global issue. However, India’s rates are significantly higher than in comparable middle-income countries, and the reasons are deeply structural, dietary, and cultural. Understanding these drivers is essential for both clinicians designing interventions and patients trying to reverse their own muscle loss.
India’s Chronic Protein Deficiency
The recommended dietary protein intake for a healthy adult is 0.8–1.0 g per kg of body weight per day. For active individuals and those over 40, the target rises to 1.2–1.6 g/kg/day. However, a 2020 IMRB survey found that 73% of Indian households are protein-deficient, with the average Indian consuming approximately 0.6 g/kg/day, barely half the minimum recommended amount.
This deficiency is not simply about poverty or food access. Instead, it reflects deeply embedded dietary patterns across all income levels. India’s predominantly vegetarian or semi-vegetarian diet, heavy in refined carbohydrates like rice, roti, and processed snacks, provides insufficient high-quality protein for adequate muscle protein synthesis. Consequently, even well-nourished, middle-class Indian adults routinely fall far short of the protein needed to maintain lean muscle.

Sedentary Urban Lifestyles and Muscle Disuse
Muscle mass is maintained through mechanical loading, in simpler terms, through physical use. Without regular resistance-type activity, muscle fibres shrink in a process called disuse atrophy. Moreover, the rate of disuse atrophy accelerates with age: after 30, sedentary individuals can lose 3–5% of their muscle mass per decade. After 60, that rate doubles.
India’s rapid urbanisation has created a generation of desk-bound professionals with minimal incidental physical activity. Specifically, India’s IT, banking, and service sectors employ tens of millions involve 8–10 hours of seated, screen-based work daily. Furthermore, the cultural conflation of physical fitness with vanity means that resistance training, the most effective intervention for muscle preservation, is widely avoided by the very population that needs it most.
The Thin-Fat Indian Phenotype and Hidden Muscle Loss
Research by Professor C.S. Yajnik at KEM Hospital, Pune, established that South Asians, including Indians, carry significantly less muscle and more fat at the same body weight compared to Western populations. This “thin-fat” phenotype means that a 40-year-old Indian man with a BMI of 23 may carry clinically low skeletal muscle mass alongside elevated visceral fat, yet appear entirely healthy on standard assessments.
Consequently, this phenotype makes standard screening tools essentially useless for detecting muscle loss in Indian patients. BMI rises when you gain muscle and falls when you lose it, providing actively misleading information. In contrast, body composition analysis measures muscle directly, in kilograms, compared against age- and sex-adjusted Indian population norms.
The Awareness Gap: Muscle Health Is Not on the Radar
The InBody-Ipsos study found that awareness of muscle health and its consequences is critically low across India. Most respondents associated muscle only with athletics or bodybuilding, not with metabolic health, immunity, or disease prevention. As a result, the majority of people losing muscle are doing so completely unaware, with no monitoring, no intervention, and no clinical flag.
Furthermore, most standard health check-ups in India even at premium corporate wellness programmes, do not include body composition assessment. They measure weight, BMI, and blood markers. However, none of these detects skeletal muscle mass directly. In other words, the health system itself creates a systematic blind spot around the very marker that most needs monitoring.
How InBody Detects Muscle Loss That Blood Tests Cannot
Detecting muscle loss accurately requires measuring it directly. This is precisely what InBody’s Direct Segmental Multi-frequency Bioelectrical Impedance Analysis (DSM-BIA) does. In under 60 seconds, standing barefoot on the device and holding the hand electrodes, a patient receives a complete body composition profile, no radiation, no blood draw, no specialist required.
The Muscle-Specific Markers InBody Measures
Several InBody measurements are directly relevant to muscle health assessment in Indian clinical practice. Each one provides information that weight, BMI, and blood tests cannot supply.
- Skeletal Muscle Mass (SMM): Total lean muscle in kilograms, compared against the population norm for the patient’s age, sex, and height. This is the primary marker of muscle health, and the one that 71% of Indians fall below.
- Skeletal Muscle Index (SMI): Appendicular muscle mass divided by height squared. This is the standard AWGS metric for sarcopenia diagnosis. InBody calculates it automatically and flags patients below the Asian threshold.
- Segmental Lean Analysis: Muscle mass broken down by right arm, left arm, trunk, right leg, and left leg. This reveals which segments have the greatest deficit, particularly the leg muscle, which is the primary site of glucose disposal and the first muscle group to deteriorate with inactivity.
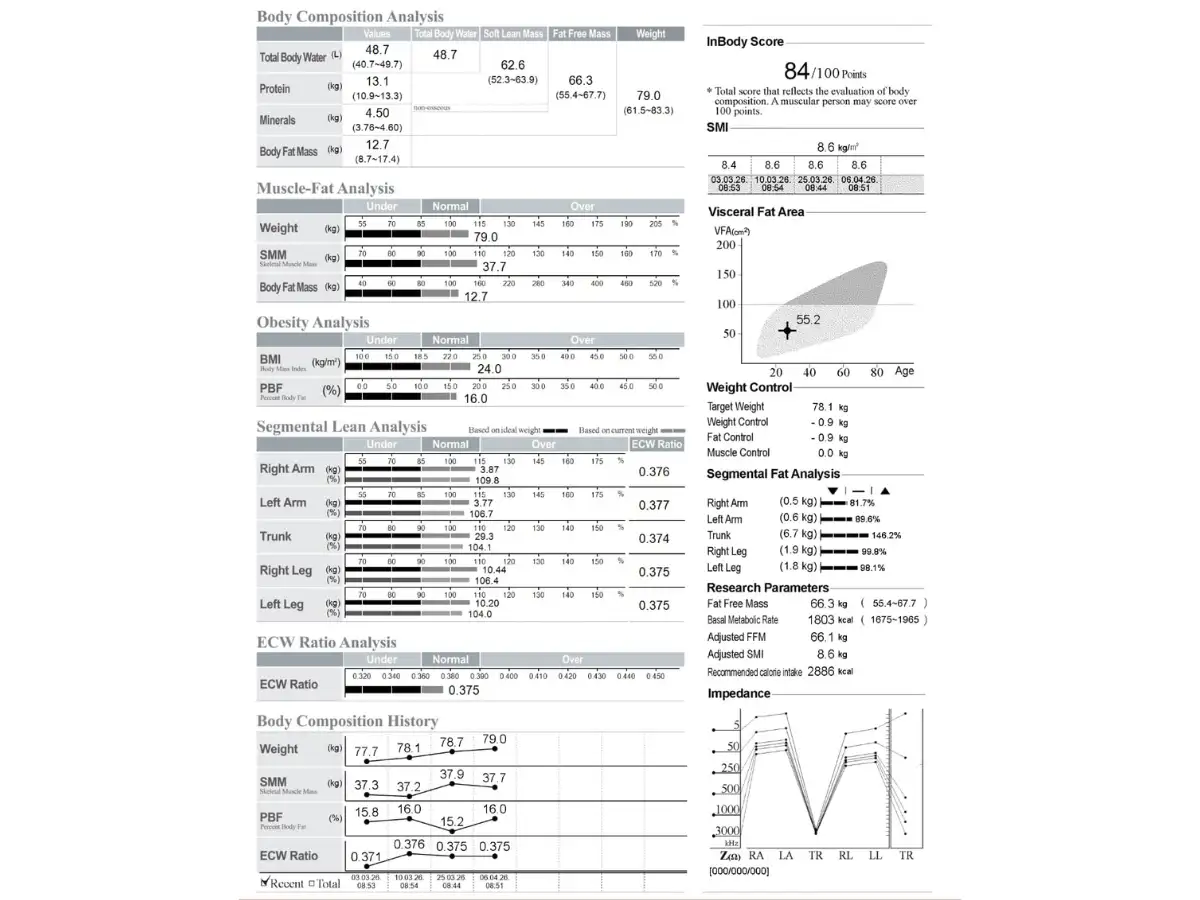
- InBody Score: A composite 0–100 index of overall muscle-fat balance. It provides a single trackable number that motivates patients and makes compliance measurable over time.
- ECW/TBW Ratio: Extracellular water to total body water, a marker of inflammation and cellular health that rises in patients with chronic low-grade metabolic dysfunction, which commonly accompanies muscle loss in Indian adults.
CLINICAL PROTOCOL FOR MUSCLE MASS SCREENING
For Indian adult patients aged 30 and above, the following InBody monitoring schedule is recommended for proactive muscle health management:
Baseline scan → at first presentation or annual health check
3-month scan → to assess response to initial nutrition and exercise intervention
6-month scan → to confirm sustained muscle gain and fat reduction trajectory
Annual scan → ongoing metabolic risk monitoring
Markers to track at every visit: SMM vs age norm · SMI vs AWGS threshold · Segmental Lean (legs specifically) · ECW/TBW ratio · InBody Score trajectory over time.
Real-World Case: Catching Muscle Loss Before the Diagnosis
A 44-year-old male IT professional in Bengaluru presented to a corporate wellness clinic with persistent fatigue, mild lower back pain, and borderline fasting glucose of 101 mg/dL. His BMI was 24.2 normal by standard criteria. As a result, he had never been flagged for metabolic risk by previous health assessments.
An InBody 770 scan told a different clinical story. Specifically, it revealed Skeletal Muscle Mass 4.1 kg below the population norm for his age and height, a Skeletal Muscle Index of 6.8 kg/m² below the AWGS sarcopenia threshold of 7.0 kg/m², Visceral Fat Level 11 (high risk range), and an ECW/TBW ratio of 0.391, indicating subclinical inflammation. In other words, he met clinical criteria for sarcopenia at 44 with normal BMI and no prior detection.
Consequently, a 16-week targeted programme was initiated: resistance training three times per week, dietary protein increased to 1.4 g/kg/day using eggs, paneer, and whey protein, and Vitamin D supplementation. At the 16-week follow-up scan, results were clinically significant across every tracked marker:
| +3.2 kg Skeletal Muscle Mass gained | 7.4 kg/m² SMI, now above AWGS sarcopenia threshold | ↓3 units Visceral Fat Level (11 → 8) | 94 mg/dL Fasting glucose at 16 weeks back to normal range |
In addition, his fatigue resolved completely, and his back pain improved, both consequences of improved core and lower limb muscle mass. This case reflects a pattern seen consistently across Indian clinical and corporate wellness settings: muscle loss is widespread, largely undetected, and highly reversible when identified early.
5 Practical and Evidence-Based Ways to Reverse Muscle Loss in India
The good news is that muscle loss is not inevitable. In fact, it is one of the most reversible metabolic conditions in medicine, provided it is caught early and addressed with the right combination of nutrition, exercise, and monitoring. The following five steps represent the strongest available evidence for reversing muscle loss specifically in Indian adults.
Way 1: Fix Your Protein Intake First, It Is the Foundation of Everything
No exercise programme can build or preserve muscle without adequate dietary protein. The minimum target for an adult Indian is 1.0 g of protein per kilogram of body weight per day. For those over 40, recovering from illness, or actively trying to rebuild muscle, the target rises to 1.2–1.6 g/kg/day. In practice, for a 70 kg Indian adult, this means 70–112 g of protein daily, roughly double what most Indians currently consume.
Moreover, protein quality matters as much as quantity. Complete proteins containing all nine essential amino acids are particularly effective at stimulating muscle protein synthesis. Specifically, the best Indian sources include eggs (the benchmark complete protein), paneer, curd, chicken, fish, soya chunks, and dal combined with rice. Furthermore, protein should be distributed across all three meals rather than concentrated in a single sitting, as muscle protein synthesis responds to per-meal amino acid exposure.

Way 2: Begin Progressive Resistance Training, Three Sessions Per Week Is Enough
Resistance training is the most powerful stimulus for skeletal muscle protein synthesis available. Moreover, it does not require a gym, equipment, or a personal trainer. Bodyweight exercises, such as squats, lunges, push-ups, planks, and step-ups provide sufficient mechanical load to drive meaningful muscle growth in previously sedentary individuals. Specifically, three sessions per week of 30–40 minutes each is the minimum effective dose for measurable muscle gain in Indian adults.
Furthermore, the principle of progressive overload, gradually increasing the challenge by adding repetitions, sets, or resistance over time, is essential for sustained results. Without progression, adaptation plateaus within 6–8 weeks. Additionally, resistance training provides benefits beyond muscle mass: it reduces visceral fat, improves insulin sensitivity, strengthens bone density, and significantly reduces cardiovascular risk, all of which are particularly relevant to the Indian metabolic profile.
Way 3: Measure Muscle Mass Directly, Stop Relying on Weight and BMI
You cannot manage what you cannot measure. This principle is especially true for muscle mass, because the standard tools that Indian adults use to track their health, weighing scales and BMI are structurally incapable of measuring muscle. In fact, BMI actively misleads: it rises when you gain muscle and falls when you lose it, making it counterproductive as a progress tool for anyone improving their body composition.
Instead, body composition analysis using InBody should form the baseline of any muscle health programme. A scan takes under 60 seconds, is non-invasive, radiation-free, and delivers all five key muscle health markers immediately. Moreover, serial scanning every 8–12 weeks provides the objective trend data that motivates continued adherence and allows clinicians to catch early plateaus or losses before they become clinically significant.
FOR CLINICIANS: INTEGRATING InBody INTO STANDARD CARE
InBody scans are now deployed at corporate wellness clinics, endocrinology units, bariatric centres, physiotherapy facilities, and sports medicine departments across India, including Apollo Hospital Chennai, Fortis hospitals, and Max Healthcare. For practices not yet equipped, InBody India provides a facility-finder tool at inbody. This allows you to refer patients directly to a nearby scanning centre.
Way 4: Address Vitamin D and Micronutrient Deficiencies
Vitamin D plays a direct role in skeletal muscle protein synthesis and muscle fibre composition. Specifically, Vitamin D receptors are present in muscle cells, and deficiency leads to reduced Type II muscle fibre size, the fast-twitch fibres responsible for strength and power. Furthermore, Vitamin D deficiency is estimated to affect 50–90% of Indian adults, despite India’s abundant sunlight, due to indoor lifestyles, sun avoidance, and low dietary sources.
Beyond Vitamin D, magnesium, zinc, and B12 deficiencies are also highly prevalent in India and all three are directly involved in muscle protein synthesis and neuromuscular function. Therefore, a basic micronutrient panel should accompany any body composition assessment in Indian adults presenting with low muscle mass. Correcting these deficiencies, combined with protein and resistance training, significantly accelerates the rate of muscle recovery.
Way 5: Track Your InBody Score and Make It Your Health Benchmark
The InBody Score is a composite 0–100 index of overall muscle-fat balance. A score above 80 indicates a healthy body composition. Scores below 70 indicate a clinically relevant imbalance, typically too much fat, too little muscle, or both simultaneously. Critically, this single number makes body composition tangible, trackable, and motivating for patients who struggle to interpret raw data.
In practice, patients who receive and understand their InBody Score show significantly better compliance with nutrition and exercise programmes than those who receive only weight or BMI data. Moreover, the score tracks the effect of both interventions simultaneously, showing whether a patient is losing fat, gaining muscle, or achieving the optimal combination of both. Consequently, it is particularly valuable in Indian clinical settings where patient compliance and follow-up are among the most significant barriers to achieving lasting health outcomes.
Who Should Be Screened for Muscle Mass Loss in India?
Given that 71% of Indian adults already have poor muscle health, the practical answer is: almost everyone over 30 should have a baseline body composition scan. However, the following groups have the highest clinical priority for immediate screening and intervention.
- Adults over 30 with sedentary occupations: IT professionals, office workers, and others with minimal daily physical activity are at the highest risk of progressive disuse atrophy, often without any obvious symptoms until the loss is clinically significant.
- Patients with prediabetes or Type 2 diabetes: Low muscle mass both causes and accelerates insulin resistance. Body composition monitoring should be standard in every diabetic patient’s care plan, not an optional add-on.
- Patients with unexplained fatigue, weakness, or reduced exercise tolerance: These are frequently the first symptoms of muscle loss, particularly in the 40–60 age group, and are routinely missed by standard blood panels.
- Adults over 50, all genders: The rate of muscle loss accelerates sharply after 50. Sarcopenia screening using InBody SMI data should be integrated into all preventive health assessments in this age group.
- Post-surgical and post-illness patients: Hospitalisation, bed rest, and reduced oral intake drive rapid muscle loss. Serial InBody monitoring during rehabilitation tracks recovery and guides nutritional support precisely.
- Women post-menopause: Oestrogen plays a protective role in muscle mass maintenance. Its withdrawal at menopause accelerates muscle loss significantly, making this group a high-priority target for proactive body composition monitoring.
Frequently Asked Questions
According to the InBody–Ipsos Study 2020, 71% of Indians aged 30–55 have poor muscle health, with muscle loss starting in the late 20s among sedentary individuals, and due to the thin-fat Indian phenotype, this low muscle mass often goes unnoticed because it can occur even in people with normal body weight.
Protein provides the building blocks for muscle, but only when combined with resistance training does it effectively stimulate muscle growth and increase measurable muscle mass.
Adequate protein intake (1.2–1.6 g/kg/day) combined with progressive resistance training three times a week can lead to measurable increases in skeletal muscle mass on InBody scans within 8–12 weeks, with individuals below normal muscle levels often gaining about 1.5–3.5 kg over 12–24 weeks.
InBody scanning is a quick (under 60 seconds), non-invasive, and radiation-free test that is safe for most patients—including those with diabetes, heart disease, kidney disease, or cancer—except for individuals with implanted electronic devices (like pacemakers or ICDs) and pregnant women, while results in patients with severe oedema should be interpreted along with their clinical fluid status.
InBody scanners are available in hospitals, fitness centres, corporate wellness clinics, and sports medicine facilities across major Indian cities like Mumbai, Delhi, Bengaluru, Chennai, Hyderabad, and Pune—with scans completed in under 60 seconds and instant results on a printed report via inbody.in.
Key Takeaways for Clinicians and Patients
- 71% of Indians aged 30–55 have poor muscle health, confirmed by the InBody-Ipsos study of 1,243 adults across 8 Indian cities in 2020.
- Low skeletal muscle mass is an independent risk factor for Type 2 diabetes, metabolic syndrome, sarcopenia, immune dysfunction, and cardiovascular disease, not merely a fitness concern.
- BMI and weight measurements cannot detect muscle loss. InBody body composition analysis measures skeletal muscle mass directly, in kilograms, against age- and sex-adjusted Indian norms.
- India’s muscle loss crisis is driven by three structural factors: chronic protein deficiency (73% of households), sedentary urban lifestyles, and the thin-fat Indian phenotype that hides muscle loss behind normal body weight.
- Muscle loss is highly reversible with consistent resistance training (3×/week) and adequate protein (1.0–1.6 g/kg/day), producing measurable InBody gains of 1.5–3.5 kg of skeletal muscle mass within 12–24 weeks.
- The five evidence-based steps to reverse muscle loss: fix protein intake ·start resistance training · measure with InBody · address micronutrient deficiencies · track your InBody Score over time.
Find Out Where You Stand: Before the Loss Becomes the Diagnosis
An InBody scan takes under 60 seconds and gives you and your doctor the precise muscle health data that no blood test, weight reading, or BMI calculation can provide.

Find an InBody Scanner Near You
References & Clinical Sources
- InBody and Ipsos. “71% Indians suffer from poor muscle health.” Joint study across 8 Indian cities, n=1,243. November 2020.
- Asian Working Group for Sarcopenia. “2019 Consensus Update on Sarcopenia Diagnosis and Intervention.” Journal of the American Medical Directors Association. 2020.
- DeFronzo RA, et al. “Skeletal muscle insulin resistance is the primary defect in type 2 diabetes.” Diabetes Care. 2009.
- Yajnik CS, Yudkin JS. “The Y-Y paradox.” The Lancet. 2004;363(9403):163.
- Misra A, et al. “Consensus statement for diagnosis of obesity and metabolic syndrome for Asian Indians.” JAPI. 2009.
- Kim TN, Choi KM. “Sarcopenia: Definition, epidemiology, and pathophysiology.” Journal of Bone Metabolism. 2013.
- InBody Co. “Validation of InBody BIA against DEXA in diverse clinical populations.” InBody White Paper Series. Seoul: InBody Co., 2022.
- Neeland IJ, et al. “Visceral and ectopic fat, atherosclerosis, and cardiometabolic disease.” Obesity Reviews. 2019.
- International Diabetes Federation. IDF Diabetes Atlas, 10th Edition. Brussels: IDF, 2021.
- WHO Expert Consultation. “Appropriate body-mass index for Asian populations.” The Lancet. 2004;363(9403):157–163.

Most trending articles

InBody vs DEXA vs Skinfold Calipers: Which Body Composition Test Is Right for You in India?
DEXA scans, InBody BIA, skinfold calipers — three different ways to measure body composition. Accuracy comparisons, cost in India, accessibility, and which method makes sense for your specific goal.

Skinny Fat in India: Why 40% of Normal Weight Indians Have Dangerously High Body Fat
India's hidden obesity epidemic. Skinny fat (TOFI — Thin Outside, Fat Inside) affects millions of normal-weight Indians. How body composition testing reveals what BMI hides — and the exact protocol to fix it.

Healthy Body Composition by Age for Indians: Reference Ranges at 20s, 30s, 40s, 50s+
Body composition reference ranges for Indian men and women by age. Find out if your body fat %, muscle mass, and visceral fat level are healthy for your age and what to do if they're not.