You can be slim, have a normal BMI, and still be silently accumulating dangerous visceral fat because the tissue responsible for burning it is disappearing. Here is the clinical evidence, and what to do about it.
- 71% Indians aged 30–55 have poor muscle health, InBody-Ipsos, 2020, 80%
- Of insulin-stimulated glucose uptake handled by skeletal muscle
- 3–5% Muscle mass lost per decade after age 30 in sedentary individuals
- 17.5% Indians under 65 are already meeting clinical sarcopenia criteria (AWGS)
Note for Medical Practitioners
This article draws on the InBody-Ipsos 2020 study (n=1,243, 8 Indian cities, age 30–55), peer-reviewed sarcopenia and visceral adiposity literature, and AWGS 2019 consensus guidelines. InBody metrics cited SMM, SMI, VFL, PBF, ECW/TBW are produced by Direct Segmental Multi-frequency BIA validated at 98.4% accuracy against DEXA. All clinical references are listed at the end of this article.
The Hidden Fat Problem No Standard Test Detects
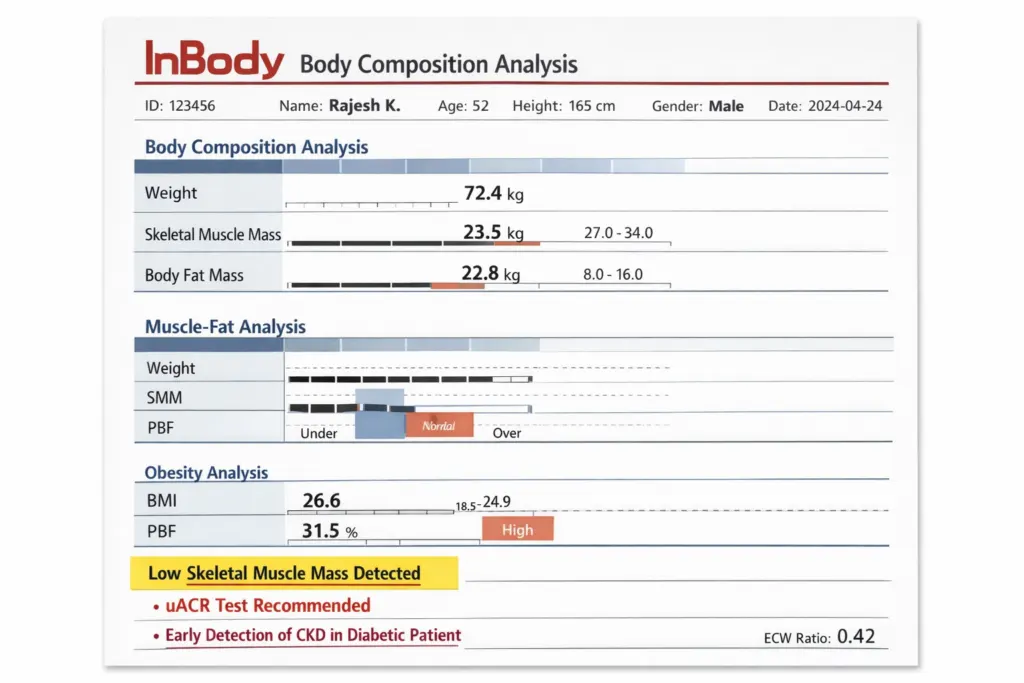
Imagine a 42-year-old woman in Pune. Her weight is 58 kg, BMI is 22.8, textbook normal, fasting glucose is borderline at 98 mg/dL, and lipids are slightly elevated. Her doctor tells her to “watch her diet.” No further investigation is done.
What a standard health check-up missed: her visceral fat level is 14 in the high-risk range. Her skeletal muscle mass is 3.8 kg below the norm for her age and height. Her ECW/TBW ratio is 0.394, indicating subclinical inflammation. She has the thin-fat Indian phenotype, high hidden fat, low muscle, entirely normal-looking by standard metrics.
This is not an edge case. The InBody-Ipsos 2020 study across 1,243 Indian adults aged 30–55 in eight cities found that 71% had poor muscle health. And the biological mechanism connecting muscle loss to fat gain is now well-established in the clinical literature, yet barely reflected in routine Indian healthcare practice.
The Biology: How Skeletal Muscle Controls Fat Storage
Skeletal muscle is not passive structural tissue. It is a metabolically active endocrine organ that directly governs whether energy is burned or stored as fat. To understand the connection between muscle loss and hidden fat growth, you need to understand three mechanisms.
Mechanism 1: Basal Metabolic Rate and Energy Disposal
Skeletal muscle accounts for approximately 40% of total body mass in a healthy adult and contributes disproportionately to resting energy expenditure. A kilogram of muscle burns roughly 13 kcal per day at rest compared to approximately 4.5 kcal per kilogram of fat. Therefore, when muscle mass declines, Basal Metabolic Rate (BMR) falls proportionally.
For a 70 kg Indian adult who loses 4 kg of skeletal muscle over a decade of sedentary living, this translates to a resting metabolic deficit of roughly 50 kcal per day, not dramatic in isolation, but compounded over years, it creates a sustained caloric surplus that the body preferentially deposits as visceral fat.
Mechanism 2:Glucose Disposal and Insulin Resistance
Skeletal muscle handles 80% of insulin-stimulated glucose uptake in the postprandial state. This is well-established in the foundational work of DeFronzo et al. (Diabetes Care, 2009). When muscle mass is insufficient, this primary glucose disposal pathway is structurally compromised regardless of body weight or dietary intake.
The result is compensatory hyperinsulinaemia. The pancreas secretes more insulin to force glucose clearance. Chronically elevated insulin is itself a potent driver of adipogenesis, particularly visceral fat deposition. So low muscle mass does not just fail to burn fat; it actively signals the body to create more of it.
Mechanism 3: Myokine Signalling and Lipolysis
Active skeletal muscle secretes myokines, signalling molecules including IL-6, irisin, and FGF21 that directly stimulate fat oxidation in adipose tissue, improve hepatic lipid metabolism, and suppress visceral fat expansion. When muscle mass is low and physical activity is minimal, myokine output collapses. The anti-fat-storage signalling that muscle provides is simply absent.
This is a relatively recent understanding in metabolic medicine and is part of why skeletal muscle is now accurately described as an endocrine organ, not merely a mechanical one.
| Mechanism | What Happens When Muscle Is Low? | Outcome: Detectable | le via InBody? |
|---|---|---|---|
| BMR Reduction | Resting energy expenditure falls; caloric surplus accumulates | Visceral fat deposition | ✅ SMM vs norm |
| Impaired Glucose Disposal | 80% glucose uptake pathway compromised → hyperinsulinaemia | Adipogenesis, T2DM risk | ✅ SMM + VFL |
| Myokine Deficit | Irisin, IL-6, FGF21 collapse → fat oxidation halted | Visceral fat expansion | ✅ Segmental Lean + ECW/TBW |
| Disuse Atrophy Loop | Fat infiltrates the muscle compartment (myosteatosis) → further weakness | Sarcopenic obesity | ✅ PBF + SMI |
Why India’s Hidden Fat Problem Is Uniquely Dangerous
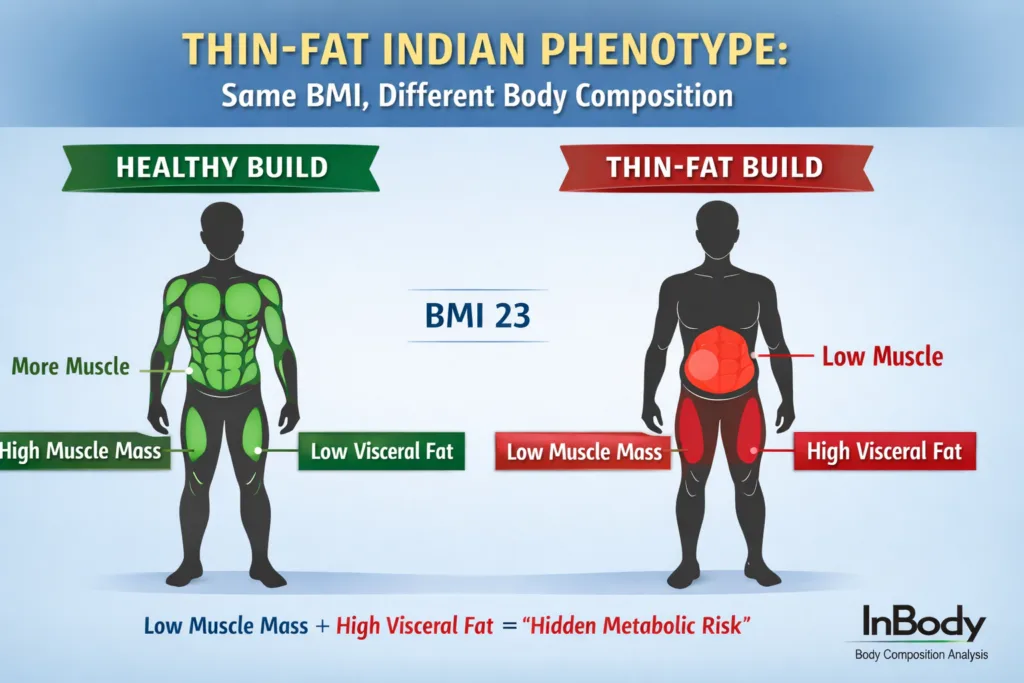
Professor C.S. Yajnik at KEM Hospital Pune described the “Y-Y paradox” (Lancet, 2004): South Asians carry significantly less lean mass and more body fat at the same BMI as European counterparts. An Indian man with a BMI of 23 may carry the metabolic risk equivalent of a European man at a BMI of 27.
This thin-fat Indian phenotype means that the standard tools used in Indian health assessments, weighing scales, BMI, and waist circumference, systematically underestimate both the muscle deficit and the visceral fat load. The two problems co-exist silently, masked by “normal” aggregate metrics.
Furthermore, India’s structural factors compound the biological risk. A 2020 IMRB survey found that 73% of Indian households are protein-deficient, with average consumption at 0.6 g/kg/day barely half the minimum recommended intake for muscle maintenance. Combined with sedentary urban occupations and a cultural discomfort with resistance training, the conditions for progressive muscle loss and hidden fat accumulation are endemic.
How InBody Detects What Blood Tests Cannot
Detecting the muscle–fat imbalance that drives hidden fat growth requires measuring both simultaneously, directly, with segmental precision. This is exactly what InBody’s Direct Segmental Multi-frequency Bioelectrical Impedance Analysis (DSM-BIA) provides in under 60 seconds, without radiation, without a blood draw, at the point of clinical care.
The InBody Markers That Map Muscle Loss to Fat Risk
- Skeletal Muscle Mass (SMM): Total lean muscle in kg, compared against age- and sex-adjusted Indian norms. The primary marker of fat-burning capacity and metabolic engine size.
- Visceral Fat Level (VFL): A 1–20 scale measuring abdominal visceral adipose tissue. Levels above 10 are associated with significantly elevated cardiometabolic risk. This is the “hidden fat” that BMI cannot detect.
- Skeletal Muscle Index (SMI): Appendicular lean mass ÷ height². The AWGS 2019 diagnostic criterion for sarcopenia is below 7.0 kg/m² in men, 5.4 kg/m² in women, using Asian-specific thresholds.
- Segmental Lean Analysis: Muscle mass broken down by right arm, left arm, trunk, right leg, and left leg. The primary site of glucose disposal, the leg muscle deficit, is identifiable segment by segment.
- ECW/TBW Ratio: Extracellular water to total body water. A value above 0.390 indicates subclinical inflammation, which accompanies sarcopenic obesity and correlates with visceral fat expansion.
- InBody Score: A 0–100 composite index of overall muscle-fat balance. Scores below 70 indicate a clinically relevant imbalance of too much fat, too little muscle, or both.
Clinical Protocol Muscle-Fat Screening Schedule (Indian Adults 30+)
- Baseline scan at first presentation or annual health check. Record SMM, VFL, SMI, ECW/TBW, and InBody Score.
- 3-month scan assess response to initial nutrition and resistance training intervention. Flag any SMM loss or VFL increase immediately.
- 6-month scan confirm sustained muscle gain and visceral fat reduction trajectory.
- Annual scan ongoing metabolic risk monitoring. Compare against previous scans, not population norms alone.
Markers to track at every visit: SMM vs age norm · SMI vs AWGS threshold · Segmental Lean (legs) · VFL · ECW/TBW ratio · InBody Score trend.
Real-World Case: Two Problems Caught With One Scan
A 47-year-old female HR director in Mumbai presented for a corporate wellness assessment. Her weight was 61 kg. BMI: 23.4. Blood pressure: normal. Fasting glucose: 105 mg/dL (borderline). She complained of persistent fatigue and difficulty losing weight despite “eating well.”
An InBody 270 scan revealed:
- Skeletal Muscle Mass: 3.6 kg below the norm for her age, sex, and height
- Visceral Fat Level: 13 (high-risk range; threshold is 10)
- Skeletal Muscle Index: 5.1 kg/m² below the AWGS sarcopenia threshold of 5.4 kg/m²
- ECW/TBW ratio: 0.396 (elevated inflammation marker)
- InBody Score: 62 clinically significant imbalance
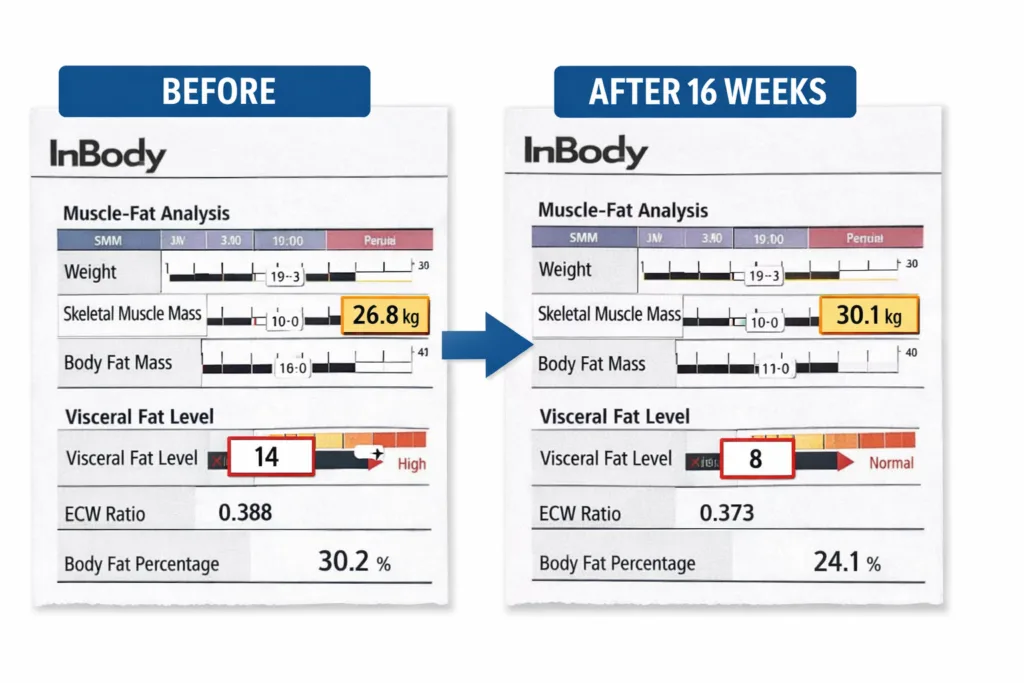
A targeted 16-week programme was initiated: resistance training three times per week, dietary protein increased to 1.3 g/kg/day using eggs, Greek yoghurt, paneer, and chicken, and Vitamin D supplementation (baseline level was 14 ng/mL). At 16 weeks, her InBody results were unambiguous.
- +2.9 kg Skeletal Muscle Mass gained in 16 weeks
- VFL 9 Visceral Fat Level down from 13 to 9, now below risk threshold
- 5.7 SMI kg/m² is now above the AWGS sarcopenia threshold of 5.4
- 96 mg/dL Fasting glucose at 16 weeks back within normal range
Her fatigue resolved, and her InBody Score rose from 62 to 79. Critically, her weight on the scale changed by only 1.2 kg, an imperceptible shift that would have told her doctor nothing. The simultaneous muscle gain and visceral fat reduction were only visible through body composition analysis.
5 Evidence-Based Steps to Build Muscle and Defeat Hidden Fat
The biological strategy against hidden fat growth is not complicated, but it requires addressing both sides of the muscle-fat equation simultaneously. The following five steps represent the strongest available clinical evidence for Indian adults.
1. Set a Protein Target, Then Hit It Every Day
The minimum for muscle maintenance in a healthy Indian adult is 1.0 g/kg/day. For those over 40, actively rebuilding, or post-illness: 1.2–1.6 g/kg/day. For a 65 kg woman, that is 65–104 g daily, roughly double the national average. Distribute across all three meals; muscle protein synthesis responds to per-meal amino acid exposure. Best Indian sources: eggs, Greek yoghurt, paneer, chicken, fish, soya chunks, dal + rice combined.
2. Begin Progressive Resistance Training 3 Sessions Per Week
Resistance training is the most potent stimulus for skeletal muscle protein synthesis and the most direct intervention against visceral fat accumulation. Three 30–40 minute sessions per week is the minimum effective dose. Bodyweight is sufficient to start: squats, lunges, push-ups, step-ups, and planks provide enough mechanical load. Apply progressive overload increase repetitions, sets, or resistance every 2–3 weeks to prevent adaptation plateau.
3. Replace BMI With Body Composition Measurement
BMI rises when you gain muscle and falls when you lose it. It cannot distinguish between a 70 kg individual with excellent body composition and one with sarcopenic obesity; both return the same number. InBody DSM-BIA takes under 60 seconds, requires no blood draw, and delivers SMM, VFL, SMI, ECW/TBW, and InBody Score immediately. Serial scanning every 8–12 weeks gives the objective trend data to confirm or adjust your intervention.
4. Test and Correct Vitamin D, Magnesium, Zinc, and B12
Vitamin D receptors are present in skeletal muscle cells. Deficiency reduces Type II muscle fibre size, the fast-twitch fibres critical to strength and metabolic activity. Vitamin D deficiency affects an estimated 50–90% of Indian adults despite abundant sunlight, due to indoor lifestyles. Magnesium, zinc, and B12 are cofactors in muscle protein synthesis and neuromuscular function. A basic micronutrient panel should accompany any body composition assessment in low-SMM patients.
5. Track Your InBody Score as Your Health Benchmark
The InBody Score (0–100) encodes muscle-fat balance into a single trackable number. Above 80: healthy composition. Below 70: clinically relevant imbalance. Patients who receive and understand their InBody Score show significantly better adherence to nutrition and exercise programmes than those given only weight or BMI data because the score makes the biology tangible, measurable, and responsive to action.
Who in India Should Be Screened Right Now
Given that 71% of working-age Indians already have poor muscle health, the pragmatic answer is: any adult over 30 who has not had a body composition assessment should have one. The following groups, however, carry the highest clinical priority.
- Adults over 30 with sedentary occupations (IT, banking, services): Disuse atrophy begins silently. Symptoms typically only appear when 20–30% of muscle mass is already gone.
- Patients with prediabetes or Type 2 diabetes: Low SMM both causes and accelerates insulin resistance. Body composition monitoring should be standard in every diabetic care plan.
- Adults with normal or low BMI but elevated triglycerides or fasting glucose: This pattern strongly suggests that the thin-fat phenotype body composition analysis will confirm it.
- Women post-menopause: Oestrogen withdrawal accelerates muscle loss significantly. VFL often rises sharply at menopause even without dietary changes.
- Post-surgical and post-hospitalisation patients: Bed rest drives rapid muscle catabolism. Serial InBody monitoring tracks recovery and guides nutritional repletion precisely.
- Any adult with unexplained fatigue, weakness, or difficulty losing weight despite caloric restriction: These are the classic presentations of sarcopenic obesity, confirmed in minutes by an InBody scan.
For Clinicians: Integrating InBody Into Standard Practice
InBody scanners are deployed at major Indian health systems, including Apollo Hospital Chennai, Fortis hospitals, Max Healthcare, and across corporate wellness clinics, endocrinology units, bariatric centres, physiotherapy facilities, and sports medicine departments nationwide.
For practices not yet equipped, InBody India provides a facility-finder at inbody.in allowing direct patient referral to a nearby scanning centre. Clinic and hospital procurement enquiries: inbody.in/contact-us.
Frequently Asked Questions
Q. What exactly is “Hidden Fat,” and why is it dangerous?
Hidden fat, scientifically known as Visceral Fat, wraps around your internal organs rather than sitting just under the skin. Unlike subcutaneous fat, it is “biologically active,” secreting hormones and inflammatory markers that significantly increase the risk of type 2 diabetes and heart disease, even if you look “thin” on the outside.
Q. How does a “Biological Strategy” differ from a standard diet?
A standard diet focuses on total weight loss (the number on the scale), which often leads to the loss of both fat and muscle. A biological strategy uses Body Composition Analysis to ensure you are specifically targeting fat mass while preserving or building the muscle tissue that drives your metabolism.
Q. Why is “Biological Precision” necessary for long-term success?
The body is an adaptive machine. If you cut calories too low, your body lowers its Basal Metabolic Rate (BMR) to survive. By using precision data to track your muscle-to-fat ratio, you can adjust your nutrition to “feed the muscle” and “starve the fat,” preventing the dreaded metabolic crash.
Q. How does the InBody scan reveal what my eyes can’t see?
The InBody uses Bioelectrical Impedance Analysis (BIA) to measure how much of your weight is water, muscle, and fat. It provides a “Visceral Fat Level” score. Tracking this number is the absolute best way to guarantee that your biological strategy is working, even when the mirror doesn’t show it yet.
Key Takeaways
- Hidden visceral fat grows when skeletal muscle is low through three mechanisms: reduced BMR, impaired glucose disposal, and collapsed myokine signalling. This is a biological relationship, not a lifestyle observation.
- 71% of Indians aged 30–55 have poor muscle health, confirmed by the InBody-Ipsos 2020 study across 8 cities and 1,243 adults. The muscle crisis is mainstream, not marginal.
- The thin-fat Indian phenotype makes standard screening useless. BMI, body weight, and waist circumference systematically miss the co-occurrence of low SMM and high VFL that is endemic in Indian adults.
- InBody body composition analysis detects both problems simultaneously in under 60 seconds, measuring SMM, VFL, SMI, segmental lean, ECW/TBW, and InBody Score against age- and sex-adjusted Indian norms.
- The biological strategy to defeat hidden fat growth: fix protein (1.0–1.6 g/kg/day) · start resistance training (3×/week) · replace BMI with InBody body composition assessment · correct Vitamin D and micronutrients · track InBody Score every 8–12 weeks.
- The intervention works. Consistent resistance training + protein optimisation produces 1.5–3.5 kg SMM gain and 2–4 VFL unit reduction within 12–16 weeks, confirmed by serial InBody scans.
Find Out Where You Stand Before the Fat Becomes the Diagnosis
An InBody scan takes under 60 seconds and gives you and your doctor the precise muscle and visceral fat data that no blood test, weight reading, or BMI calculation can provide.

Find an InBody Scanner Near You →
Enquire for Your Clinic →
References & Clinical Sources
- InBody and Ipsos. “71% Indians suffer from poor muscle health.” Joint study across 8 Indian cities, n=1,243. November 2020.
- Asian Working Group for Sarcopenia. “2019 Consensus Update on Sarcopenia Diagnosis and Intervention.” JAMDA. 2020.
- DeFronzo RA et al. “Skeletal muscle insulin resistance is the primary defect in type 2 diabetes.” Diabetes Care. 2009.
- Yajnik CS, Yudkin JS. “The Y-Y paradox.” The Lancet. 2004;363(9403):163.
- Misra A, et al. “Consensus statement for diagnosis of obesity and metabolic syndrome for Asian Indians.” JAPI. 2009.
- Kim TN, Choi KM. “Sarcopenia: Definition, epidemiology, and pathophysiology.” Journal of Bone Metabolism. 2013.
- Neeland IJ, et al. “Visceral and ectopic fat, atherosclerosis, and cardiometabolic disease.” Obesity Reviews. 2019.
- InBody Co. “Validation of InBody BIA against DEXA in diverse clinical populations.” InBody White Paper Series. 2022.
- International Diabetes Federation. IDF Diabetes Atlas, 10th Edition. Brussels: IDF, 2021.